")
Back to Journals » Clinical Ophthalmology » Volume 18
Tolerability of Current Treatments for Dry Eye Disease: A Review of Approved and Investigational Therapies
Authors Gupta PK , Toyos R, Sheppard JD, Toyos M , Mah FS, Bird B, Theriot PE , Higgins D
Received 21 February 2024
Accepted for publication 6 July 2024
Published 16 August 2024 Volume 2024:18 Pages 2283—2302
DOI https://doi.org/10.2147/OPTH.S465143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tolerability of current treatments for dry eye disease – Video abstract [465143]
Views: 97
Preeya K Gupta,1,2 Rolando Toyos,3 John D Sheppard,4 Melissa Toyos,3 Francis S Mah,5 Brian Bird,6 Pamela E Theriot,7 Don Higgins8
1Triangle Eye Consultants, Raleigh, NC, USA; 2Department of Ophthalmology, Tulane University, New Orleans, LA, USA; 3Toyos Clinic, Nashville, TN, USA; 4Virginia Eye Consultants, Norfolk, VA, USA; 5Scripps Clinic, La Jolla, CA, USA; 6Department of Ophthalmology, Eastern Virginia Medical School, Norfolk, VA, USA; 7Lusk Eye Specialists, Shreveport, LA, USA; 8Dry Eye Treatment Center of Connecticut, Plainville, CT, USA
Correspondence: John D Sheppard, Virginia Eye Consultants, 241 Corporate Blvd, Norfolk, VA, USA, Tel +1 757 622-2200, Fax +1 757 622-4866, Email [email protected]
Abstract: Dry eye disease (DED) is a common, multifactorial ocular disease impacting 5% to 20% of people in Western countries and 45% to 70% in Asian countries. Despite the prevalence of DED and the number of treatment approaches available, signs and symptoms of the disease continue to limit the quality of life for many patients. Standard over-the-counter treatment approaches and behavior/environmental modifications may help some cases but more persistent forms often require pharmacological interventions. Approved and investigational pharmaceutical approaches attempt to treat the signs and symptoms of DED in different ways and tend to have varying tolerability among patients. While several pharmacological approaches are the standard for persistent and severe disease, mechanical options provide alternate treatment modalities that attempt to balance efficacy and comfort. Newer approaches target the causes of DED, utilizing novel delivery methods to minimize irritation and adverse events. Here, we review approved and investigational approaches to treating DED and compare patient tolerability.
Keywords: dry eye disease, tolerability, safety, pharmaceutical interventions, mechanical interventions
Introduction
Dry eye disease (DED), or keratoconjunctivitis sicca, is a common, multifactorial ocular disease impacting between 5% and 20% of people in Western countries and between 45% and 70% of people in Asian countries.1,2 The pathophysiology of DED involves a cascade of inflammatory events that can be worsened by intrinsic factors such as age, sex, and autoimmune diseases.1,3 Desiccating stress at the ocular surface and tear hyperosmolarity, which can be caused by extrinsic factors, activate mitogen-activated protein kinase signaling; upregulate nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3 (NLPR3) and toll-like receptor and oxidative stress pathways; and stimulate the secretion of cytokines, chemokines, and matrix metalloproteinases. This initiates a vicious inflammatory cycle that leads to disruption of the epithelial barrier, apoptosis of epithelial cells in the cornea and lacrimal gland cells, and T-cell infiltration. This loss of homeostasis in the cornea, conjunctiva, and lacrimal glands causes further instability of the tear film, which in turn triggers further inflammatory signaling.3 The loss of tear film homeostasis and accompanying ocular symptoms, including tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities, play etiologic roles in DED.4 The onset of DED may be influenced by many variables, including local ocular factors, systemic diseases, sociodemographic characteristics, environmental conditions, elective medications, and surgical procedures.5 Additionally, DED is cyclical, with symptom flares and inactive periods.6
There is no gold standard sign or symptom for diagnosing DED. Instead, a combination of questionnaires and evaluations are used to identify DED (Table 1). Symptoms of DED include ocular pain, burning, dryness, foreign body sensation, and visual disturbances.1 Signs of DED include decreased noninvasive break-up time; elevated or a large interocular disparity in osmolarity; or positive ocular surface staining of the cornea, conjunctiva, or lid margin.4 Additionally, gentle expression of the meibomian glands and meibography may be used as assessment tools.7 These methods can determine the presence of meibomian gland dysfunction by assessing the quantity of meibum secreted as well as alterations in its lipid composition and its expressibility. Meibography also evaluates meibomian gland loss, demonstrated by gland dropout and changes in its length, thickness, and density.8,9
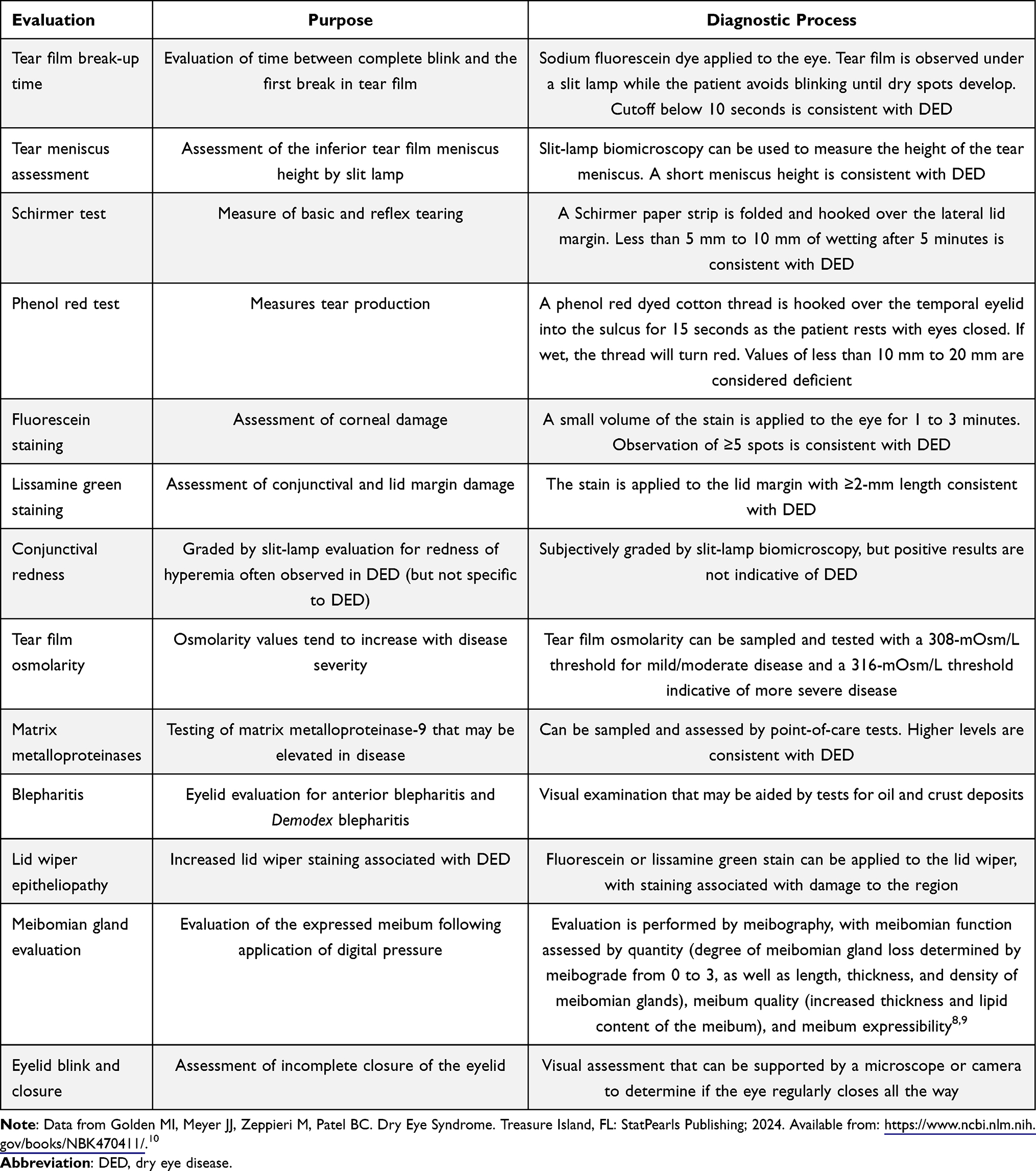 |
Table 1 Most Frequently Used Methods for Diagnosing DED |
According to the Tear Film and Ocular Surface Society Dry Eye Workshop II (TFOS DEWS II) report, the first step for staged management and treatment of DED involves educating the patient on the condition, its management, and its prognosis.4 Ocular lubricants, such as artificial tears, and lid hygiene/warm compresses can be used to relieve DED symptoms.4 Patients should modify the local environment and remove or change any potential aggravators of the disease.4 Changing or supplementing a diet with foods rich in omega-3, omega-6, and omega-7 polyunsaturated fatty acids has anti-inflammatory effects and may be associated with clinical improvement in DED, both independently and in addition to other therapies.11–16 If these initial modifications do not improve the signs and symptoms of DED, over-the-counter and prescription medications may be used (Table 2).4
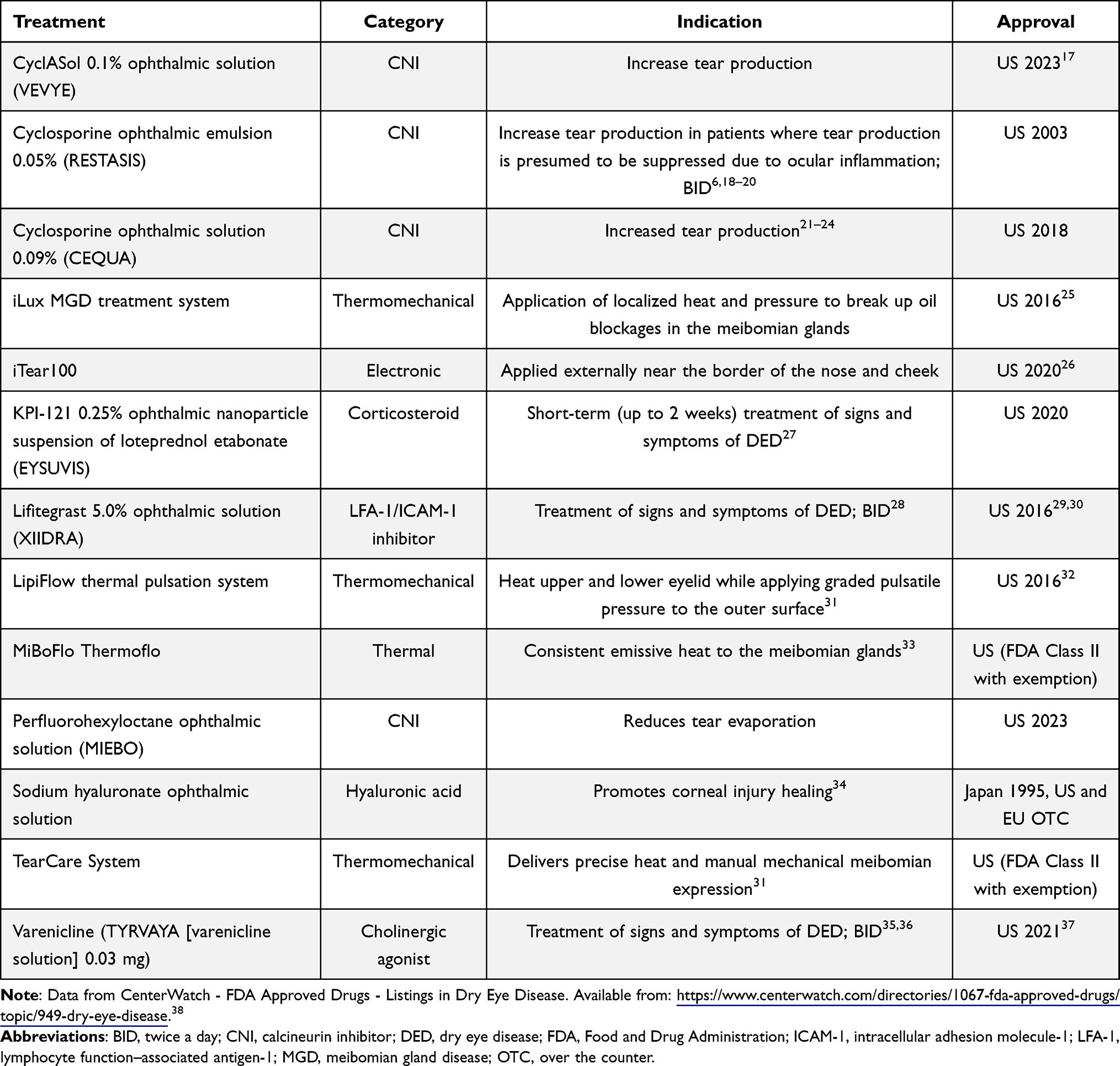 |
Table 2 List of Approved Treatments for DED in the US |
Many of the therapeutic options for DED have issues with tolerability (such as instillation-site burning or pain and blurred vision), which impacts the quality of life (QoL) for patients and may lead to decreased adherence.6 This review focuses on the tolerability profiles of the US Food and Drug Administration (FDA)-approved and investigational products designed to treat the underlying causes of DED and highlights the educational points that may improve patient adherence and outcomes.
Currently Approved Pharmacological Treatments for Dry Eye Disease
DED is classified by the TFOS DEWS II report into 3 subtypes: evaporative dry eye (EDE), the most common form; aqueous-deficient dry eye (ADDE); and a mixed form of DED when these 2 etiologies co-occur.4 ADDE is characterized by insufficient tear production by the lacrimal glands leading to a reduced aqueous component in the tear film, while EDE stems primarily from dysfunction of the meibomian glands that results in deficient secretion of the lipid component of the tear film.4,39
All forms of DED can be treated with tear substitutes, topical lubricants, and anti-inflammatory drugs, including steroids and cyclosporine.4,39,40 Therapeutic strategies specifically targeting EDE include enhanced lid hygiene using warm compresses, lid scrubs, and gentle massage for instance, and mechanical methods to unclog blocked meibomian glands, such as thermal pulsation (TPS), intense pulsed light (IPL), and meibomian gland probing.9 Additionally, antibiotics such as topical azithromycin or oral doxycycline can be used to treat EDE.9,41 For the treatment of severe ADDE, secretagogues can be used to stimulate tear production by acting on the ocular surface receptors.40
Treatment of DED involves a comprehensive approach of treating the underlying stressors/causes of the disease (if possible) by simple nonprescription therapies (lid cleansers, warm compresses, and nutraceuticals) before using more invasive/pharmacological treatments (Table 3).42 Because of the heterogeneity in the population of patients with DED and the variability in severity and character of the disease in these patients, there is no clearly delineated treatment regimen for DED. Instead, treatment of DED can involve multiple recommended therapeutic approaches that can be selected based on the nature and degree of the disease, as well as other individual factors.4 Initial treatments such as artificial tears provide short-term symptom relief by coating the corneal surface and creating an unbroken layer to protect the eye from desiccating stress and injury.1,43 However, these treatments merely address symptoms of DED and have no direct effect on the underlying inflammation or mechanisms responsible for disease progression.
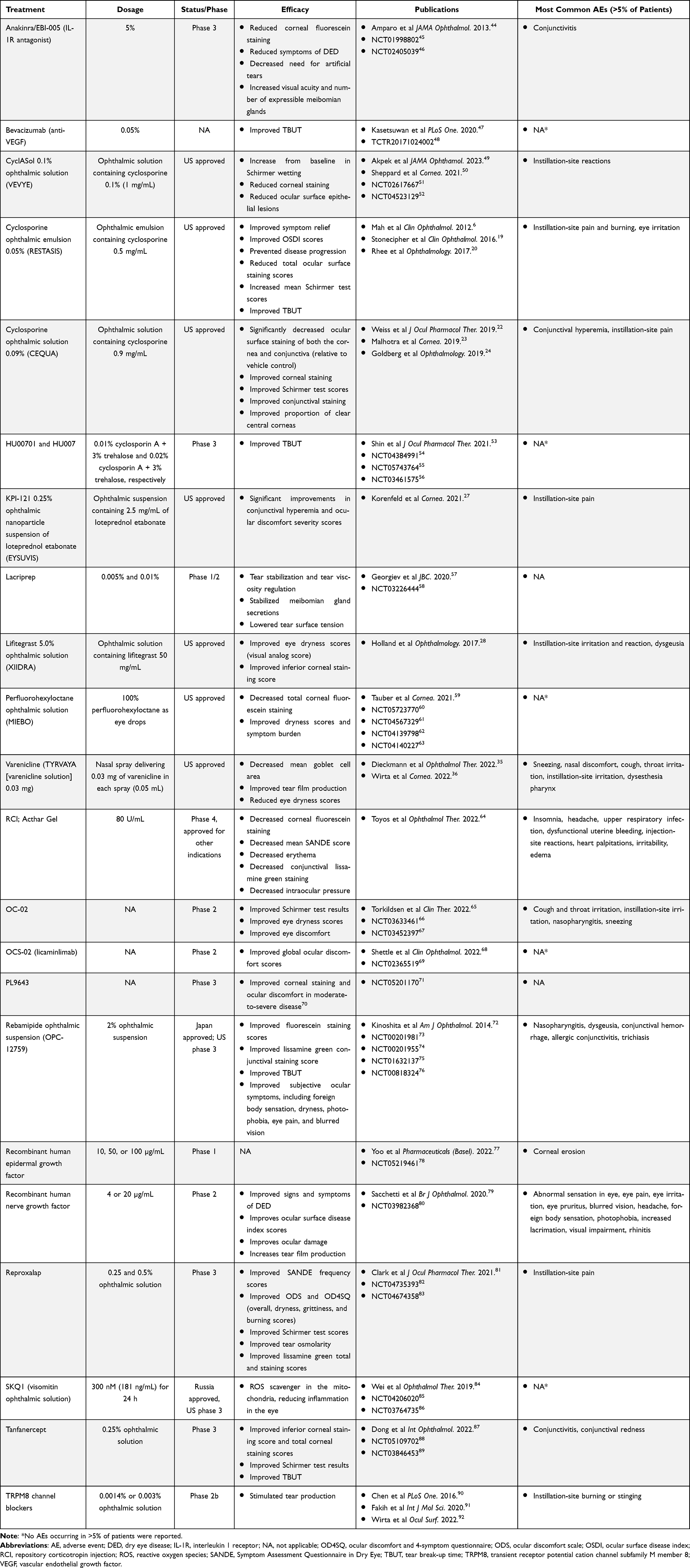 |
Table 3 Summary of Efficacy for Approved and Investigational DED Treatments |
A wide range of artificial tear formulations are commercially available and are commonly based on cellulose derivatives, povidone, polyvinyl alcohol, carbomers, or hyaluronic acid. The type of patients’ tear film deficiency can guide the selection of artificial tear formulations based on the type of lubricant they contain, which can be aqueous or lipid based.39,93 For instance, in patients with meibomian gland dysfunction, lipid-containing artificial tears are recommended.93 However, artificial tears or ocular lubricants may include preservatives or excipients like benzalkonium chloride that cause irritation and ultimately worsen DED.39,94,95 For patients with severe DED, autologous serum eyedrops are indicated.93 These are derived from a patient’s own serum, which has a similar composition and biochemical properties as tears and contains growth factors and inflammatory substances that promote epithelial healing.96
When therapeutic strategies using simple nonprescription therapies and artificial tears are not sufficient to address symptoms of DED, alternative approaches involving prescription treatments can be adopted. Among these available prescription therapies are topical corticosteroids, which improve the signs and symptoms of DED but are relatively unsuitable for long-term use due to the associated side effects of prolonged exposure, including elevated intraocular pressure (IOP), glaucoma, and cataracts.1,6,97–99 EYSUVIS (0.25% loteprednol etabonate ophthalmic suspension; Alcon Laboratories, Inc, Fort Worth, TX, USA) is a topical corticosteroid approved by the US FDA in 2020 for short-term (2 week) treatment of the signs and symptoms of DED.100,101 Loteprednol uses mucus-penetrating particle technology to improve ocular drug delivery and reduce DED flares by modulating the proinflammatory signaling mediated by the glucocorticoid receptor.27,102,103 Across 4 clinical studies (one phase 2 and three phase 3 studies), 1430 patients with DED treated with loteprednol 4 times a day for 2 weeks demonstrated significant improvements in conjunctival hyperemia and ocular discomfort severity scores.27,102 Additionally, 12.9% (185/1430) of loteprednol-treated patients reported an adverse event (AE) with 8.5% (121/1430) reporting a treatment-related AE. The most frequently occurring treatment-emergent AE (TEAE) was instillation-site pain (5.2%).27 Although the majority of AEs were mild to moderate in severity, 0.6% (8/1430) of patients reported a severe AE, including instillation-site pain. Mean IOP values were similar in patients treated with loteprednol and vehicle, and 0.6% of patients in the loteprednol treatment group experienced an IOP measurement of ≥21 mm Hg in 1 or both eyes compared to 0.3% of patients in the vehicle treatment group.27
For patients suffering from chronic DED, several pharmacological treatment options that are better suited for long-term treatment are available. These include anti-inflammatory agents such as topical cyclosporine or lifitegrast, the cholinergic agonist varenicline, the immunomodulatory hormonal treatment repository corticotropin injection (RCI), or the perfluorohexyloctane ophthalmic solution MIEBO.17,18,21,29,37,104–106
Cyclosporine A (CsA) is a calcineurin inhibitor that mitigates the immune response and is indicated for transplantation, rheumatoid arthritis, psoriasis, and amyotrophic lateral sclerosis.107 Topical CsA reduces the expression of interleukin-2 and its receptors in T cells, which decreases their proliferation, inhibits cell-mediated inflammatory pathways in the eye (inhibiting calcineurin), and helps restore the ocular surface.1,43,108 As a result, continued use of topical CsA may increase tear production and reduce the signs and symptoms of DED.22 Approved CsA formulations in the US include cyclosporine ophthalmic solution 0.09% (CEQUA; Sun Pharmaceutical Industries, Inc., Princeton, NJ, USA; referred to as OTX-101 0.09%), cyclosporine ophthalmic solution 0.05% (RESTASIS; Allergan, Inc., Irvine, CA, USA), and CyclASol 0.1% ophthalmic solution (VEVYE; Novaliq GmbH, Heidelberg, Germany; Table 2).17,18,21,109 The first generic form of RESTASIS, cyclosporine ophthalmic emulsion 0.05% single-use vials, was approved by the US FDA in 2022 (Viatris, Inc., Canonsburg, PA, USA).110 An additional formulation, cyclosporine ophthalmic emulsion 0.1% (Verkazia; Santen Pharmaceutical Co., Ltd, Emeryville, CA, USA), is approved by the US FDA for vernal keratoconjunctivitis, a rare ocular allergy condition.104 OTX-101 0.09% (cyclosporine solution) is a nanomicellar, clear aqueous solution of CsA approved by the US FDA in August 2018 for keratoconjunctivitis sicca.21,22 Cyclosporine ophthalmic emulsion 0.05% was approved by the US FDA in 2003 for DED.111 CyclASol 0.1% ophthalmic solution is a clear, topical, water-free ophthalmic solution of CsA in a novel, semifluorinated alkane (SFA)-based EyeSol technology vehicle, using the SFA perfluorobutylpentane. CyclASol increases bioavailability of CsA while avoiding the use of oils, surfactants, and preservatives.50,112
All 3 formulations of cyclosporine approved by the US FDA demonstrated efficacy in treating DED symptoms compared to vehicle. In a pooled analysis of a phase 2b/3 and a phase 3 study assessing the efficacy and safety of OTX-101 0.09% compared to vehicle, the primary endpoint of a ≥10-mm increase from baseline in Schirmer test scores at Day 84 was met. Patients treated with OTX-101 0.09% experienced a significant increase in tear production compared to vehicle-treated patients (16.6% of eyes vs 9.0% of eyes, respectively; P <0.0001), as well as a significantly greater change from baseline in total corneal fluorescein staining for all common post-baseline time points (Day 28, 56, and 84; P ≤0.0013).23 In a phase 4 open-label study evaluating cyclosporine ophthalmic emulsion 0.05%, patients had significantly decreased total ocular surface and corneal staining scores after 6 months of treatment with cyclosporine 0.05% (P <0.001). Patients also experienced a significant increase in mean average eye Schirmer test scores from 5.3 mm at baseline to 8.7 mm at the 6-month time point (P = 0.010).19 In the phase 2b/3 ESSENCE study assessing the efficacy and safety of CyclASol 0.1%, the primary endpoint was met, with a statistically greater improvement from baseline in total corneal fluorescein staining in patients treated with CyclASol compared to vehicle at Week 4 (P = 0.0002). There was no significant difference in a >10-mm increase from baseline in Schirmer test scores between patients treated with CyclASol 0.1% and vehicle.50
Overall, these formulations of cyclosporine were well tolerated with mild AEs. In a phase 2b/3 and phase 3 study, TEAEs for patients receiving OTX-101 0.09% (n = 523) were mostly mild to moderate and resolved without treatment.23 There were no clinically significant changes from baseline in visual acuity or IOP.23 The most common AE in the OTX-101 0.09% arm was instillation-site pain, experienced by 24.2% of patients.24 The most common ocular TEAEs included conjunctival hyperemia (30/372 [8.1%]), blepharitis (5/372 [1.3%]), eye irritation (3/372 [0.8%]), eye pruritus (1/372 [0.3%]), and foreign body sensation (1/372 [0.3%]). There were no ocular-related serious AEs (SAEs) reported.24 In four phase 2 and 3, multicenter, randomized, controlled clinical studies (n = 1200), the most commonly reported AE was ocular burning (204/1200 [17%]).18,113 Other commonly reported AEs include conjunctival hyperemia, discharge, epiphora, eye pain, foreign body sensation, pruritis, stinging, and visual disturbances (blurring).18 An open-label phase 4 study found similar safety events, with the most commonly reported ocular AEs including instillation-site burn (3/40 [7.5%]), instillation-site pain (3/40 [7.5%]), and eye irritation (2/40 [5%]), with 1 patient experiencing a treatment-related nonocular TEAE (headache).19 In a phase 2b/3 study, patients receiving CyclASol had similar proportions of ocular TEAEs (20/162 [12.3%]) vs patients receiving vehicle (14/166 [8.4%]).50 The most frequently occurring ocular TEAEs were reduced visual acuity (CyclASol, 5/162 [3.1%]; vehicle, 3/166 [1.8%]), instillation-site pain (CyclASol, 4/162 [2.5%]; vehicle, 2/166 [1.2%]), and blurred vision (CyclASol, 2/162 [1.2%]; vehicle, 4/166 [2.4%]).50 A second phase 3 study demonstrated similar safety profiles and proportions of TEAEs further supporting the use of CyclASol for DED.49
Beyond the various CsA formulations, there are several other approved pharmacological treatments for chronic DED. Lifitegrast ophthalmic solution 5.0% (XIIDRA; Bausch & Lomb, Laval, Canada) is a small-molecule lymphocyte function–associated antigen 1 (LFA-1) antagonist approved for the treatment of signs and symptoms of DED.29,114 Lifitegrast is thought to reduce inflammation in DED by preventing T-cell activation and recruitment through the inhibition of interactions between LFA-1 and the adhesion receptor intercellular adhesion molecule 1.114 In the confirmatory OPUS-3 studies (N = 711),28 patients receiving lifitegrast had a greater mean improvement from baseline at Day 42 for itching, foreign body sensation, and eye discomfort than those receiving vehicle.28 In a pooled analysis of 5 trials, most TEAEs were mild to moderate, with 1% of lifitegrast-treated patients reporting severe ocular TEAEs vs 0.4% receiving vehicle.115 The drop comfort score identified worse scores over the first 3 minutes postinstillation followed by improvements thereafter, persisting to subsequent visits.28,116 The most frequently reported ocular TEAEs included irritation, reaction, and pain at the instillation site; there were no serious ocular TEAEs.115 Dysgeusia was the most common nonocular TEAE, reported by 14.5% (186/1287) of patients.115 Overall, 1.6% of patients reported a serious nonocular TEAE; however, none were believed to be related to the randomized treatment.115 Ninety patients (7%) receiving lifitegrast discontinued the trials.115 In the SONATA study, approximately twice as many patients receiving lifitegrast had decreased visual acuity compared to patients receiving vehicle per patient reporting, though changes through Day 360 were minimal (as assessed by 0.7 logarithm of the minimum angle of resolution best corrected visual acuity).117 Fewer patients in the lifitegrast group used artificial tears after Day 14, though use of artificial tears correlated to increased TEAEs.117
Varenicline solution 0.03 mg (TYRVAYA; Oyster Point Pharma Inc., Princeton, NJ, USA) is a small-molecule nicotinic acetylcholine (nACh) receptor partial agonist that targets and binds free nerve endings in the nasociliary and maxillary branches of the trigeminal nerve (via the nasal cavity).35,37 The binding of varenicline to nACh receptors activates the trigeminal parasympathetic pathway, which is thought to increase tear production by stimulating the autonomic nerves of the cells in the lacrimal functional unit.35,37 In a phase 2 study (n = 12), there were no ocular TEAEs, and the nonocular TEAEs were nonserious and mild in severity.35 Additionally, the incidence of ocular TEAEs for patients treated with varenicline solution (16.5%; n = 260) was consistent with the incidence reported for patients receiving vehicle (16.3%; n = 251; ONSET-2). Sneezing was the most common TEAE, occurring in 82% of patients across the ONSET-1, ONSET-2 (phase 3), and MYSTIC (phase 2) studies.118,119 Across all 3 studies, there were no SAEs resulting in study discontinuation.36,118–120
RCI (Acthar Gel; Mallinckrodt Pharmaceuticals, Hampton, NJ, USA) is a mixture of porcine adrenocorticotropic hormone analogs and pituitary peptides that bind to and activate melanocortin receptors throughout the body, including those located on the cells of the retina, and is believed to exert immunomodulatory effects on B cells, T cells, and macrophages.64,121 RCI is currently approved for severe, acute, and chronic allergic and inflammatory processes involving the eye.106 In a phase 4 pilot study (N = 15) for DED, RCI was generally effective and well tolerated, with no ocular AEs reported and 2 patients discontinuing due to other AEs.64
MIEBO (perfluorohexyloctane ophthalmic solution) consisting of inert and anhydrous SFA (Bausch & Lomb, Vaughan, Canada) is a preservative-free ophthalmic solution that rapidly spreads across the ocular surface due to its low surface/interfacial tension and interacts with the lipophilic portion of the tear film, preventing evaporation. It is a recently approved treatment option for DED.59,105 In a phase 3 study, 54 patients reported 122 TEAEs; the number of patients reporting at least 1 TEAE was similar between the treatment groups.122 The most common ocular TEAEs were blurred vision, eye irritation, and eye pain.122 Four patients reported SAEs, and 3 patients discontinued the study due to an AE.122
Mechanical Interventions
Nonpharmacological approaches to treating DED focus on promoting tear secretion and mobilization of meibum via thermal, light, mechanical, electrical, and combinatorial stimulation methods (Table 4). Mechanical stimulation may improve blood flow to the eye, which can promote tear secretion and improve dry eye symptoms.123,124 Thermal applications use heat, often in combination with pulsation/vibration, to soften and express meibum.84 Alternatively, external nasal nerve stimulation may be used to restore the activity of the lacrimal functional unit.125 In a study of an external nerve stimulator, patients experienced notable improvements 30 days after treatment in Schirmer test and ocular surface disease index scores. Overall, 9 of 101 (9%) patients reported AEs, with 2 mild AEs related to the study device. The most commonly reported AEs were sneezing and dizziness.125 There were no neurologic AEs or damage to the skin.125 One patient reported nasal pain but remained in the study.125
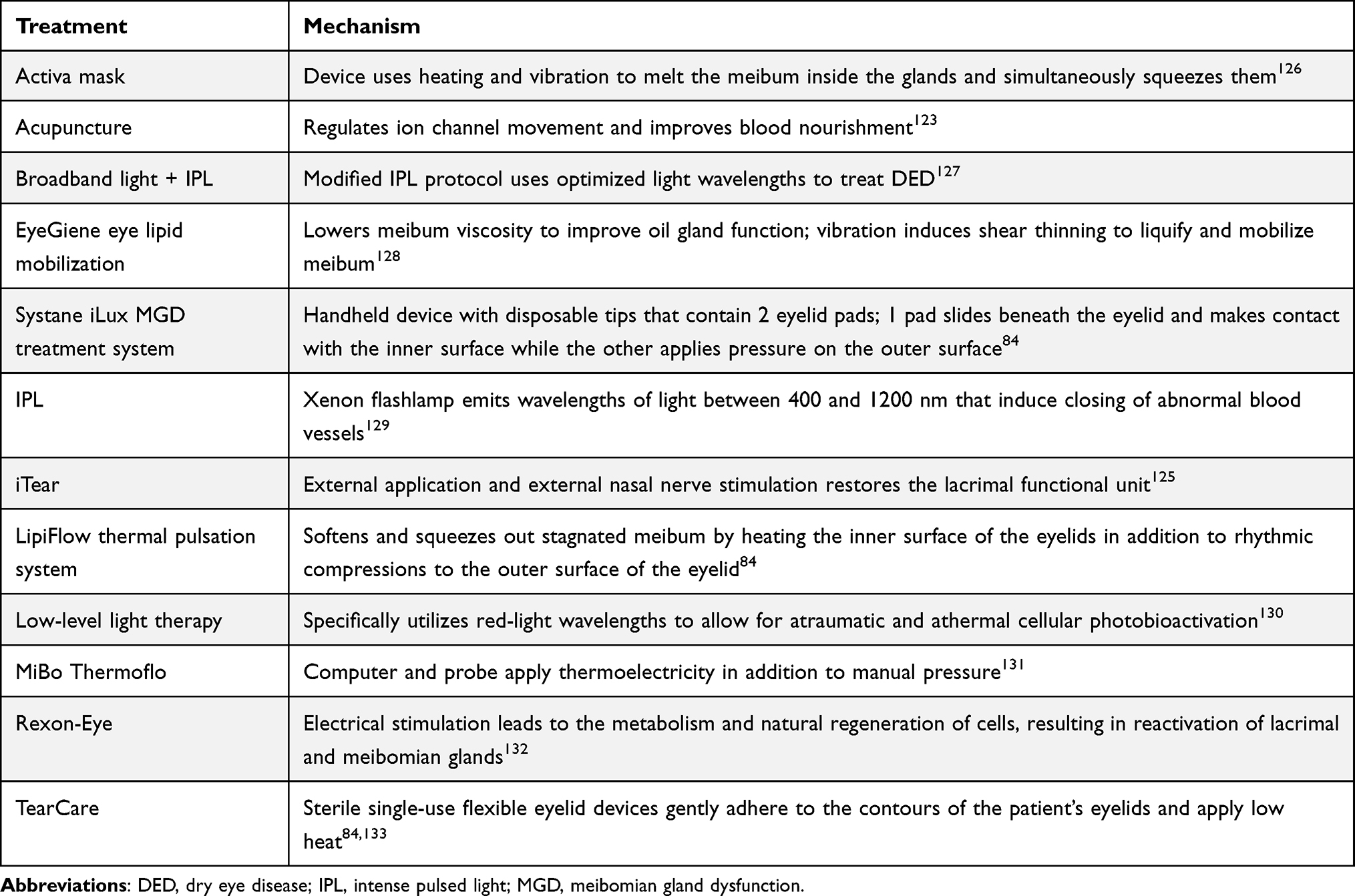 |
Table 4 Summary of Nonpharmacological Interventions for Dry Eye Disease |
IPL induces closing of abnormal blood vessels, a feature often prevalent in meibomian gland dysfunction.129 However, wavelengths emitted by IPL and those absorbed by the pigmented iris overlap, leaving patients at risk of permanent eye damage from IPL without proper eye protection.134 In a retrospective, noncomparative, interventional case series, IPL was generally well tolerated. There were no SAEs reported among the 88 patients involved. In total, 4 (8.9%) patients experienced AEs with 1 patient discontinuing the study. The AEs reported included moderate allergic conjunctivitis, moderate blepharitis (both deemed to be unrelated to the study), moderate bacterial conjunctivitis, and mild skin pain. No patients experienced systemic AEs.135
Low-level light therapy (LLLT) specifically uses red-light wavelengths, and this allows for atraumatic and athermal cellular photobioactivation.136 The red-light wavelength causes photonic interference allowing therapeutic levels of light to penetrate the skin to repair damaged cells and improve cell function.136 An evaluation using light-emitting diode-based LLLT in 20 patients found no SAEs.137 Electrotherapy delivers electrical stimulation to the biological tissue believed to stimulate metabolism and natural regeneration.132 Treatment with electrotherapy improved ocular surface disease index scores, noninvasive tear break-up time scores, and normalized tear meniscus height values.132 No AEs were noted in the study, and patients were reportedly comfortable during the procedure.132
Punctual plugs, also called lacrimal plugs, are small devices made of silicone or collagen that can be used to treat patients with severe ADDE. Punctual plugs increase tear retention on the ocular surface by occluding tear ducts, which leads to delayed tear drainage.93 In a retrospective study examining the use of silicone punctual plugs between 1996 and 2000 in 153 patients and 203 eyes, including 127 eyes with DED, symptoms improved in 73.9% of eyes at 4 ± 2 weeks’ follow-up. Additionally, mean corneal fluorescein staining scores, which assess the viability of the epithelium, significantly decreased at 4 ± 2 weeks’ follow-up (P <0.01), indicating an improvement in ocular surface disease with punctual plugs.138,139 The most common complication associated with the use of punctual plug is loss of the plug.93
Although mechanical approaches are well tolerated, cost, availability, and reproducibility tend to create substantial access burdens, and the symptom relief experienced after in-office treatment tends to decline over time, limiting long-term tolerability for patients.84,131,140 In addition to the in-office treatments, patients may perceive maintenance protocols as tedious and time consuming, which can lead to poor adherence and tolerability.140
Pharmacological Treatments in Development for Dry Eye Disease
In addition to the currently approved treatments for DED, there are other options in development. Ectoine eye drops are being evaluated to improve drug delivery and efficacy. Ectoine creates a protective hydration shell around proteins and biomolecules due to a strong binding capacity with water.141 In a systematic review of 16 studies in sensitive patient groups (ie, <18 years or after surgery), a limited number of AEs were reported and no SAEs were reported.141 Similarly, HU00701 and HU007 (0.01% CsA + 3% trehalose and 0.02% CsA + 3% trehalose; respectively; Huons Co., Ltd., Gyeonggi-do, Republic of Korea) are 2 new formulations of CsA in development.53 Similar to previous formulations of CsA, the inclusion of trehalose is intended to limit desiccation.142 Although a clinical study evaluating CsA with trehalose did not identify improved corneal staining, the treatment was deemed to be safe and well tolerated.53,143 In total, 8 patients reported AEs, including infection, eye disorder, general disorders and administration site conditions, and musculoskeletal and connective tissue disorders. The rates were consistent among the treatment, vehicle, and control groups.53 Additionally, AZR-MD-001 (Azura Ophthalmics; Tel Aviv, Israel), an ointment containing selenium sulfide, diminishes the aberrant production of keratin that clogs the meibomian glands by inhibiting the growth and development of keratinocytes. This inhibition of keratinocytes leads to a reduction in the differentiation of epidermal cells and the production of corneocytes.144 Results from a phase 2 trial show improvements in dry eye symptoms at 3 months, though 15 out of 23 AZR-MD-001-treated patients (across 3 dosage groups) reported at least 1 ocular TEAE.12
Building on the success of varenicline nasal spray, OC-02 (simpinicline solution; Viatris, Inc., Canonsburg, PA, USA) is a highly selective nACh receptor agonist. OC-02 stimulates nACh receptors on the trigeminal parasympathetic nerve in the nasal cavity to induce tear production.65 In a phase 2 study, 52% (64/123) of the patients receiving OC-02 reported a TEAE, with most of those incidents being nonocular and mild to moderate in severity (1 patient did present with a severe TEAE, but this was considered unrelated to the study).65 The ocular TEAEs included eye pruritis (1 patient) and keratitis (1 patient).65
Other novel pharmacological approaches focus on treating the mechanisms responsible for DED. Growth factors such as epidermal growth factor (EGF) or neural growth factor (NGF) are involved in many phases of growth and development and have been touted as having potential efficacy in the treatment of DED. Epidermal growth factor is a growth factor secreted from the lacrimal glands and is involved in corneal healing, suggesting a potential therapeutic role in DED.77,145 Treatment with recombinant human EGF eye drops (Daewoong Bio Inc., Seoul, Korea) was generally well tolerated with 10/36 patients in the treatment group reporting TEAEs. All reported TEAEs were mild and transient and there were no SAEs.77 Similarly, NGF plays a crucial role in modulating the central and peripheral nervous system, including the visual system.79 After treatment with recombinant human NGF eye drops (Dompé Farmaceutici S.p.A, Milan, Italy), 1 patient experienced an SAE considered unrelated to treatment but did not discontinue the study. One patient discontinued the study due to an AE of bacterial conjunctivitis.79 In the study, 29 of 40 patients experienced at least 1 AE, and 11 patients had at least 1 treatment-related AE.79 All of the AEs experienced were considered to be mild to moderate in severity, though 1 patient discontinued the treatment due to an AE.79 In general, no safety concerns emerged from this trial, with no increases in IOP or decreases in best corrected visual acuity observed and symptoms improving among those investigated on the visual analog scale.79
Reproxalap (Aldeyra Therapeutics, Inc., Lexington, MA, USA), tanfanercept (Harbour BioMed [Guangzhou] Co. Ltd., Natick, MA, USA), imatinib mesylate, (Novartis, Basel, Switzerland), licaminlimab (Novartis, Basel, Switzerland), bevacizumab (Genentech Inc., San Francisco, CA, USA), and PL9643 (Palatin Technologies, Inc., Cranbury, NJ, USA) target specific pathways in DED pathogenesis and are designed to limit the inflammatory response. Reproxalap, a reactive aldehyde species (RASP) inhibitor, is a small-molecule inhibitor engineered to block RASP signaling.81 RASP are molecules that exert proinflammatory effects by binding thiol and amino groups on receptors and kinases, thereby activating cytokines and pro-histaminic factors. The proinflammatory cascade modulated by RASP also produces inflammatory molecules such as tumor necrosis factor alpha (TNF-α) and cyclooxygenase-2, and causes cell necrosis, apoptosis, and DNA damage. Notably, levels of malondialdehyde, a common form of RASP, are elevated in patients with DED. RASP signaling inhibition by reproxalap prevents the activation of nuclear factor-κ B (NF-κB), scavenger receptor A, and inflammasomes, leading to decreased levels of cytokines and histamines.146 A preliminary trial noted improvements as early as 1 week after treatment initiation; however, there were 47 ocular TEAEs in 51 patients.81 Forty-two of the TEAEs involved ocular discomfort or pain upon instillation, but all TEAEs were transient and self-limiting.81 Similarly, tanfanercept is a molecularly engineered TNF receptor 1 fragment eye drop formulation designed to inhibit TNF-α signaling to reduce inflammation.87 One study reported equal numbers of TEAEs in tanfanercept and placebo groups; however, ocular AEs were more prevalent in the tanfanercept group with conjunctivitis and conjunctival redness being the most frequently reported.87 Imatinib mesylate is a tyrosine kinase inhibitor that preclinically is a potent discoidin domain receptor 1 inhibitor.147 In preclinical studies, imatinib reduced damage to the ocular surface and reduced accumulation of inflammatory cells, restoring structure of the conjunctival epithelium.147 In a preliminary clinical study in healthy individuals (N = 32), 4 TEAEs were reported, 3 in the imatinib mesylate groups and 1 in the placebo group; all TEAEs were mild to moderate in severity and recovered without sequelae, and there were no SAEs.147 Licaminlimab is a single-chain antibody fragment that binds and neutralizes TNF-α.68 Treatment-emergent adverse events were reported in similar numbers between the treatment group (19%) and the control group (14%).68 In the licaminlimab group, dry eye and eye pruritus were the most commonly reported TEAEs and were not reported in the control group.68 Bevacizumab (anti–vascular endothelial growth factor A [VEGF-A]) is a monoclonal antibody targeting the inflammatory response through the intended modulation of VEGF-A. Through inhibition of VEGF-A, bevacizumab may attenuate the inflammatory response, with preliminary results showing the treatment to be well tolerated (no safety events reported).47 PL9643 is a melanocortin receptor pan-agonist designed to attenuate inflammation mediated by macrophages, antigen presenting cells, and antigen-specific T cells through modulation of the melanocortin system.148 There are no reported drug-related ocular AEs or SAEs in early safety and tolerability studies.70
Future therapeutic approaches are currently being investigated in preclinical models for the treatment of DED. One of these approaches involve the use of new delivery systems for improved bioavailability and prolonged drug exposure such as nanotechnology-based systems, hydrogels, and drug-eluting contact lenses.149–151 Other strategies use regenerative medicine in an attempt to regenerate lacrimal glands by means including stem cells, allogeneic transplantation, and bioengineering.150
Dry Eye Disease and Demodex Blepharitis
A common contributor to DED is Demodex blepharitis (DB), with upwards of 60% of DED patients with meibomian gland dysfunction also having DB. The Demodex mites are a normal part of the lid flora and are the most prevalent ectoparasite on the human skin.152 Demodex brevis are linked with symptomatic meibomian gland dysfunction where they can cause blockage of the orifice. Excreta from these mites can further contribute to the blockage and incite an inflammatory response, which can lead to filling, swelling, and enlargement of the meibomian gland.152 Importantly, DED can be both a cause and an effect of blepharitis, as the tear film helps provide resistance to infection.39 Diagnosis of DB is driven by signs rather than symptoms due to the overlap with many other ocular conditions.152 As a result, DB is often under or misdiagnosed.152 Treatment of DB can include IPL, LLLT, tea tree oil, manuka honey, lid hygiene, ivermectin plus (0.1% ivermectin/1% melatonin), and the US FDA-approved ophthalmic drug TP-03, a lotilaner 0.025% ophthalmic solution (XDEMVY; Tarsus Pharmaceuticals, Inc., Irvine, CA, USA).152–157 With the high incidence of DB and observed frequency of other underlying conditions, it is important to consider and effectively treat DB to maximize outcomes and help patients better tolerate their DED treatment.158
Patient Education to Help Increase Tolerability of Dry Eye Disease Treatments
Due to the cyclic nature of DED, patients frequently discontinue treatment due to intolerance, perceived lack of effect, or a perceived resolution of signs/symptoms.159 There continues to be dissatisfaction with the time to onset of effect of treatments, and patient education and awareness of this prolonged time may overcome adherence issues.159 In a retrospective analysis of cyclosporine ophthalmic emulsion 0.05% studies, patients previously discontinuing topical CsA most frequently did so as a result of burning/stinging.6 Upon continuation of cyclosporine ophthalmic emulsion 0.05%, patients were educated on dry eye and topical CsA.6 Reinitiation of the study led to a clinical benefit in a majority (80%) of patients, though 2 patients discontinued the study within 4 weeks due to the burning sensation.6 These findings further suggest that patient education on treatment expectations and the need for continued treatment should focus on topics including disease signs and symptoms, prognosis and management, time to onset of therapy effects, proper use of the medication and the treatment regimen, and common ocular side effects, their transient nature, and how to manage them.159 Patient education on how early discontinuation can limit QoL and the importance of adhering to the treatment regimen, even when temporary relief is achieved, is necessary for improved treatment tolerability.159
Conclusion
In moving beyond artificial tears, treatments for DED focus on the multitude of complex mechanisms that may be implicated in the disease. The persistent burden on the patient and impact DED has on QoL facilitate further evaluation of increasingly effective and well-tolerated treatments. Although currently approved treatments have improved outcomes, AEs and poor tolerability mean these therapeutic options are not suitable for all patients. However, new treatments or regimens with improved AE profiles are becoming increasingly more tolerable. Additionally, educating patients on the nature of the disease as well as tools to mitigate potential treatment-related AEs will encourage patient adherence and lead to improved treatment outcomes.
Abbreviations
ADDE, Aqueous-deficient dry eye; AE, Adverse event; BID, Twice a day; CsA, Cyclosporine A; DB, Demodex blepharitis; DED, Dry eye disease; EDE, Evaporative dry eye; EGF, Epidermal growth factor; FDA, Food and Drug Administration; IOP, Intraocular pressure; IPL, Intense pulsed light; LFA-1, Lymphocyte function–associated antigen 1; LLLT, Low-level light therapy; nACh, Nicotinic acetylcholine; NGF, Neural growth factor; NLRP3, Nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3; QoL, Quality of life; RASP, Reactive aldehyde species; RCI, Repository corticotropin injection; SAE, Serious adverse event; SFA, Semifluorinated alkane; TEAE, Treatment-emergent adverse event; TFOS DEWS II, Tear Film and Ocular Surface Society Dry Eye Workshop II; TNF, Tumor necrosis factor; TNF-α, Tumor necrosis factor alpha; TPS, Thermal pulsation; VEGF-A, Vascular endothelial growth factor A.
Data Sharing Statement
Data sharing is not applicable to this article, as no data sets were generated or analyzed during the current study.
Ethics Approval and Informed Consent
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Acknowledgments
Medical writing and editorial support were provided by Chuck Blajszczak, PhD, and Juliette Bouyssou, PhD, of AlphaBioCom, a Red Nucleus company, and funded by Sun Pharma.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medical writing and editorial support and manuscript submission were funded by Sun Pharma.
Disclosure
PG is a consultant to Allergan, Alcon, Aurea, Bausch & Lomb, Johnson & Johnson Vision, Kala Pharmaceuticals, Novartis, Ocular Science, RegGenRxTree, Shire, Sight Sciences, Tarsus, TearLab, TearScience, and Zeiss. JS reports personal fees from Allergan, Alcon, Avedro, Bausch & Lomb, Claris Bio, Clementia Pharma, Dompé, EyeDetec, EyeGate, Lacrisciences, Novartis, Ocular Therapeutix, Science Based Health, Senju, Shire, Sun Pharma, TearLab, TearScience, Tissue Tech, Topcon, and TopiVert; and other fees from Alcon/Novartis, Kala Pharmaceuticals, Novaliq, Noveome, Ocular Therapeutix, Shire, TearLab, and Visus. MT reports consultant fees from Bausch & Lomb, Eyevance, Iridex, Mallinckrodt, Dompé, Sun Pharma, and Zeiss; speaker fees from Bausch & Lomb, Lumenis, Mallinkrodt, Shire, Sun Pharma, and Zeiss; research fees from Alcon, Allysta, Amber Ophthalmics, Bausch & Lomb, DigiSight, Dompé, Farmaceutici, Glaukos, Iridex, Kala Pharmaceuticals, Lumibird, Lumenis, Magellan, Mallinckrodt, MIXTO Lasering, Novartis, Ocular Tech, Oculos, Opternative, Ray, ReVitaLid, Recordati, Shire, Sun Pharma, Sylentis, and Zeiss; and miscellaneous fees from MIXTO Lasering. RT reports speaking fees from Mallinckrodt, Zeiss, Sun Pharma, and Oyster Point; consulting fees from Zeiss, Sun Pharma, and Oyster Point; and research fees from Mallinckrodt. FSM is the chief medical advisor at Kala Pharmaceuticals; reports consulting fees from Alcon, Allergan, Aldeyra, Aperta, Azura, Bausch & Lomb, Dermavent, Kiora, Iview, Johnson & Johnson Vision, Novartis, NuLids, and SightSciences; and research support from Thea, Sun Pharma, Viatris/Oyster Point, Tarsus, Mallinckrodt, Dompé, and YuYu. PT is part of the speaker bureau for Sun Pharma, Viatris Pharmaceuticals, and Lumenis; and is a faculty member for Johnson & Johnson Vision Institute, outside the submitted work. DH reports a patent “Ophthalmic Specialty Instrument for Treating Meibomian Gland Dysfunction” pending; and he is a key opinion leader for Lumenis speaking on OptiLight and OptiPlus & receiving compensation for this work. The authors report no other conflicts of interest in this work.
References
1. Baudouin C, Figueiredo FC, Messmer EM, et al. A randomized study of the efficacy and safety of 0.1% cyclosporine A cationic emulsion in treatment of moderate to severe dry eye. Eur J Ophthalmol. 2017;27(5):520–530. doi:10.5301/EJO.5000952
2. Dell SJ, Gaster RN, Barbarino SC, Cunningham DN. Prospective evaluation of intense pulsed light and meibomian gland expression efficacy on relieving signs and symptoms of dry eye disease due to meibomian gland dysfunction. Clin Ophthalmol. 2017;11:817–827. doi:10.2147/OPTH.S130706
3. Pflugfelder SC, de Paiva CS. The pathophysiology of dry eye disease: what we know and future directions for research. Ophthalmology. 2017;124(11S):S4–S13. doi:10.1016/j.ophtha.2017.07.010
4. Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II report executive summary. Ocul Surf. 2017;15(4):802–812. doi:10.1016/j.jtos.2017.08.003
5. Hasan Z. Dry eye syndrome risk factors: a systemic review. Saudi J Ophthalmol. 2021;35(2):131–139. doi:10.4103/1319-4534.337849
6. Mah F, Milner M, Yiu S, Donnenfeld E, Conway TM, Hollander DA. PERSIST: physician’s evaluation of restasis® satisfaction in second trial of topical cyclosporine ophthalmic emulsion 0.05% for dry eye: a retrospective review. Clin Ophthalmol. 2012;6:1971–1976. doi:10.2147/OPTH.S30261
7. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
8. Xiao J, Adil MY, Chen X, et al. Functional and morphological evaluation of meibomian glands in the assessment of meibomian gland dysfunction subtype and severity. Am J Ophthalmol. 2020;209:160–167. doi:10.1016/j.ajo.2019.09.005
9. Narang P, Donthineni PR, D’Souza S, Basu S. Evaporative dry eye disease due to meibomian gland dysfunction: preferred practice pattern guidelines for diagnosis and treatment. Indian J Ophthalmol. 2023;71(4):1348–1356. doi:10.4103/IJO.IJO_2841_22
10. Golden MI, Meyer JJ, Zeppieri M, Patel BC. Dry Eye Syndrome. Treasure Island, FL: StatPearls Publishing; 2024.
11. Macsai MS. The role of omega-3 dietary supplementation in blepharitis and meibomian gland dysfunction (an AOS thesis). Trans Am Ophthalmol Soc. 2008;106:336–356.
12. Downie LE, Watson SL, Tan J, Stapleton F, Bosworth C. A multicenter, double-masked, vehicle-controlled, randomized, parallel group clinical trial of AZR-MD-001 (AZR) in individuals with meibomian gland dysfunction. Invest Ophthalmol Visual Sci. 2021;62(8):1334.
13. Kimura Y, Mori D, Imada T, et al. Restoration of tear secretion in a murine dry eye model by oral administration of palmitoleic acid. Nutrients. 2017;9(4). doi:10.3390/nu9040364
14. Molina-Leyva I, Molina-Leyva A, Bueno-Cavanillas A. Efficacy of nutritional supplementation with omega-3 and omega-6 fatty acids in dry eye syndrome: a systematic review of randomized clinical trials. Acta Ophthalmol. 2017;95(8):e677–e685. doi:10.1111/aos.13428
15. Liu A, Ji J. Omega-3 essential fatty acids therapy for dry eye syndrome: a meta-analysis of randomized controlled studies. Med Sci Monit. 2014;20:1583–1589. doi:10.12659/MSM.891364
16. Aragona P, Bucolo C, Spinella R, Giuffrida S, Ferreri G. Systemic omega-6 essential fatty acid treatment and pge1 tear content in Sjogren’s syndrome patients. Invest Ophthalmol Vis Sci. 2005;46(12):4474–4479. doi:10.1167/iovs.04-1394
17. Novaliq GmbH. VEVYE (Cyclosporine Ophthalmic Solution) [Product Insert] 0.1%, for Topical Ophthalmic Use. Heidelberg, Germany: Novaliq GmbH; 2023.
18. Allergan. RESTASIS® (Cyclosporine Ophthalmic Emulsion) 0.05%. Irvine, CA: Allergan; 2016.
19. Stonecipher KG, Torkildsen GL, Ousler GW, Morris S, Villanueva L, Hollander DA. The IMPACT study: a prospective evaluation of the effects of cyclosporine ophthalmic emulsion 0.05% on ocular surface staining and visual performance in patients with dry eye. Clin Ophthalmol. 2016;10:887–895. doi:10.2147/OPTH.S101627
20. Rhee MK, Mah FS. Inflammation in dry eye disease: how do we break the cycle? Ophthalmology. 2017;124(11S):S14–S19. doi:10.1016/j.ophtha.2017.08.029
21. Sun Pharmaceutical Industries. CEQUA® (Cyclosporine Ophthalmic Solution) [Product Insert] 0.09%, for Topical Ophthalmic Use. Cranbury, NJ: Sun Pharmaceutical Industries; 2022.
22. Weiss SL, Kramer WG. Ocular distribution of cyclosporine following topical administration of OTX-101 in New Zealand white rabbits. J Ocul Pharmacol Ther. 2019;35(7):395–402. doi:10.1089/jop.2018.0106
23. Malhotra R, Devries DK, Luchs J, et al. Effect of OTX-101, a novel nanomicellar formulation of cyclosporine A, on corneal staining in patients with keratoconjunctivitis sicca: a pooled analysis of phase 2b/3 and phase 3 studies. Cornea. 2019;38(10):1259–1265. doi:10.1097/ICO.0000000000001989
24. Goldberg DF, Malhotra RP, Schechter BA, Justice A, Weiss SL, Sheppard JD. A phase 3, randomized, double-masked study of OTX-101 ophthalmic solution 0.09% in the treatment of dry eye disease. Ophthalmology. 2019;126(9):1230–1237. doi:10.1016/j.ophtha.2019.03.050
25. iLux MGD treatment system. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf17/K172645.pdf.
26. iTear100 neurostimulator. Available from: https://www.accessdata.fda.gov/cdrh_docs/reviews/DEN190026.pdf.
27. Korenfeld M, Nichols KK, Goldberg D, et al. Safety of KPI-121 ophthalmic suspension 0.25% in patients with dry eye disease: a pooled analysis of 4 multicenter, randomized, vehicle-controlled studies. Cornea. 2021;40(5):564–570. doi:10.1097/ICO.0000000000002452
28. Holland EJ, Luchs J, Karpecki PM, et al. Lifitegrast for the treatment of dry eye disease: results of a phase III, randomized, double-masked, placebo-controlled trial (Opus-3). Ophthalmology. 2017;124(1):53–60. doi:10.1016/j.ophtha.2016.09.025
29. Novartis. XIIDRA® (Lifitegrast Ophthalmic Solution) [Product Insert], for Topical Ophthalmic Use. East Hanover, NJ: Novartis; 2020.
30. Chiaradia PA, Zeman Bardeci LA, Dankert S, Mendaro MO, Grzybowski A. Hot topics in dry eye disease. Curr Pharm Des. 2017;23(4):608–623. doi:10.2174/1381612822666161208094841
31. Holland EJ, Loh J, Bloomenstein M, Thompson V, Wirta D, Dhamdhere K. A comparison of tearcare and lipiflow systems in reducing dry eye disease symptoms associated with meibomian gland disease. Clin Ophthalmol. 2022;16:2861–2871. doi:10.2147/OPTH.S368319
32. LipiFlow® thermal pulsation system. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf16/K161357.pdf.
33. Gomez ML, Afshari NA, Gonzalez DD, Cheng L. Effect of thermoelectric warming therapy for the treatment of meibomian gland dysfunction. Am J Ophthalmol. 2022;242:181–188. doi:10.1016/j.ajo.2022.06.013
34. Uchino M, Yokoi N, Shimazaki J, Hori Y, Tsubota K; On Behalf Of The Japan Dry Eye S. Adherence to eye drops usage in dry eye patients and reasons for non-compliance: a web-based survey. J Clin Med. 2022;11(2). doi:10.3390/jcm11020367
35. Dieckmann GM, Cox SM, Lopez MJ, et al. A single administration of OC-01 (varenicline solution) nasal spray induces short-term alterations in conjunctival goblet cells in patients with dry eye disease. Ophthalmol Ther. 2022;11(4):1551–1561. doi:10.1007/s40123-022-00530-x
36. Wirta D, Torkildsen GL, Boehmer B, et al. ONSET-1 phase 2b randomized trial to evaluate the safety and efficacy of OC-01 (varenicline solution) nasal spray on signs and symptoms of dry eye disease. Cornea. 2022;41(10):1207–1216. doi:10.1097/ICO.0000000000002941
37. Oyster Point Pharma, Inc. TYRVAYA™ (Varenicline Solution) Nasal Spray. Princeton, NJ, US: Oyster Point Pharma, Inc; 2021.
38. CenterWatch - FDA Approved Drugs - Listings in Dry Eye Disease. Available from: https://www.centerwatch.com/directories/1067-fda-approved-drugs/topic/949-dry-eye-disease. Accessed July 30, 2024.
39. Findlay Q, Reid K. Dry eye disease: when to treat and when to refer. Aust Prescr. 2018;41(5):160–163. doi:10.18773/austprescr.2018.048
40. Donthineni PR, Doctor MB, Shanbhag S, et al. Aqueous-deficient dry eye disease: preferred practice pattern guidelines on clinical approach, diagnosis, and management. Indian J Ophthalmol. 2023;71(4):1332–1347. doi:10.4103/IJO.IJO_2808_22
41. Foulks GN, Borchman D, Yappert M, Kim SH, McKay JW. Topical azithromycin therapy for meibomian gland dysfunction: clinical response and lipid alterations. Cornea. 2010;29(7):781–788. doi:10.1097/ICO.0b013e3181cda38f
42. Shen Lee B, Kabat AG, Bacharach J, Karpecki P, Luchs J. Managing dry eye disease and facilitating realistic patient expectations: a review and appraisal of current therapies. Clin Ophthalmol. 2020;14:119–126. doi:10.2147/OPTH.S228838
43. Burade V, Zalawadia R, Patel A, Ogundele A. Preclinical efficacy comparison of cyclosporine ophthalmic solution 0.09% vs cyclosporine ophthalmic emulsion 0.05% vs ciclosporin ophthalmic emulsion 0.1% in a NOD mouse model of dry eye disease. Clin Ophthalmol. 2020;14:2747–2755. doi:10.2147/OPTH.S259331
44. Amparo F, Dastjerdi MH, Okanobo A, et al. Topical interleukin 1 receptor antagonist for treatment of dry eye disease: a randomized clinical trial. JAMA Ophthalmol. 2013;131(6):715–723. doi:10.1001/jamaophthalmol.2013.195
45. Phase 3 study of EBI-005 in dry eye disease (EBI-005). NCT01998802. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT01998802?term=NCT01998802&rank=1.
46. Study of EBI-005 in dry eye disease (DED) (EBI-005). NCT02405039. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT02405039?term=NCT02405039&rank=1.
47. Kasetsuwan N, Chantaralawan K, Reinprayoon U, Uthaithammarat L. Efficacy of topical bevacizumab 0.05% eye drops in dry eye disease: a double-masked, randomized trial. PLoS One. 2020;15(6):e0234186. doi:10.1371/journal.pone.0234186
48. Efficacy of topical Bevacizumab in patients diagnosed with dry eye disease compared with conventional treatment. TCTR20171024002. ThaiClinicalTrials.org. Available from: https://www.thaiclinicaltrials.org/show/TCTR20171024002. Accessed July 19, 2024.
49. Akpek EK, Wirta DL, Downing JE, et al. Efficacy and safety of a water-free topical cyclosporine, 0.1%, solution for the treatment of moderate to severe dry eye disease: the ESSENCE-2 randomized clinical trial. JAMA Ophthalmol. 2023;141(5):459–466. doi:10.1001/jamaophthalmol.2023.0709
50. Sheppard JD, Wirta DL, McLaurin E, et al. A water-free 0.1% cyclosporine a solution for treatment of dry eye disease: results of the randomized phase 2b/3 essence study. Cornea. 2021;40(10):1290–1297. doi:10.1097/ICO.0000000000002633
51. CyclASol for the treatment of moderate to severe dry-eye disease (DED). NCT02617667. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT02617667. Accessed July 19, 2024.
52. ESSENCE 2: cyclASol for the treatment of signs and symptoms of dry eye disease (DED). NCT04523129. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04523129. Accessed 19 July, 2024.
53. Shin J, Rho CR, Hyon JY, Chung TY, Yoon KC, Joo CK. A randomized, placebo-controlled phase II clinical trial of 0.01% or 0.02% cyclosporin A with 3% trehalose in patients with dry eye disease. J Ocul Pharmacol Ther. 2021;37(1):4–11. doi:10.1089/jop.2020.0104
54. HU007 eye drops in patients with dry eye syndrome. NCT04384991. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04384991.
55. HU007 in patients with dry eye syndrome. NCT05743764. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05743764?term=NCT05743764&rank=1.
56. Efficacy and safety of HU007 eye drops in patients with dry eye syndrome. NCT03461575. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT03461575?term=NCT03461575&rank=1.
57. Georgiev GA, Gh MS, Romano J, et al. Lacritin proteoforms prevent tear film collapse and maintain epithelial homeostasis. J Biol Chem. 2021;296:100070. doi:10.1074/jbc.RA120.015833
58. Lacripep in subjects with dry eye associated with primary Sjögren’s syndrome. NCT03226444. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT03226444?term=NCT03226444&rank=1.
59. Tauber J, Wirta DL, Sall K, et al. A randomized clinical study (SEECASE) to assess efficacy, safety, and tolerability of NOV03 for treatment of dry eye disease. Cornea. 2021;40(9):1132–1140. doi:10.1097/ICO.0000000000002622
60. Effects of NOV03 on the tear film. NCT05723770. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05723770?term=NCT05723770&rank=1.
61. Effect of NOV03 on signs and symptoms of dry eye disease associated with meibomian gland dysfunction (Mojave study). NCT04567329. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04567329?term=NCT04567329&rank=1.
62. Perfluorohexylcotane (NOV03) for the treatment of signs and symptoms of dry eye disease associated with meibomian gland dysfunction (Gobi study). NCT04139798. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04139798?term=NCT04139798&rank=1.
63. Long-term safety and tolerability of NOV03 (perfluorohexyloctane) in subjects who completed trial NVU-003 (Kalahari study). NCT04140227. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04140227?term=NCT04140227&rank=1.
64. Toyos M, Toyos R, Jodoin B, Bunch R. Results from a prospective, open-label, phase 4 pilot study of repository corticotropin injection for moderate and severe dry eye disease. Ophthalmol Ther. 2022;11(3):1231–1240. doi:10.1007/s40123-022-00501-2
65. Torkildsen GL, Pattar GR, Jerkins G, Striffler K, Nau J. Efficacy and safety of single-dose OC-02 (simpinicline solution) nasal spray on signs and symptoms of dry eye disease: the PEARL phase II randomized trial. Clin Ther. 2022;44(9):1178–1186. doi:10.1016/j.clinthera.2022.07.006
66. Evaluation of the efficacy of OC-02 nasal spray on signs and symptoms of dry eye disease (the RAINIER study). NCT03633461. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT03633461?term=NCT03633461&rank=1.
67. Clinical trial to evaluate the efficacy of OC-02 nasal spray on signs and symptoms of dry eye disease (the PEARL study). NCT03452397. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT03452397?term=NCT03452397&rank=1.
68. Shettle L, McLaurin E, Martel J, Seaman JW, Weissgerber G. Topical anti-TNFα agent licaminlimab (OCS-02) relieves persistent ocular discomfort in severe dry eye disease: a randomized phase II study. Clin Ophthalmol. 2022;16:2167–2177. doi:10.2147/OPTH.S366836
69. LME636 in the relief of persistent ocular discomfort in subjects with severe dry eye disease. NCT02365519. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT02365519?term=NCT02365519&rank=1.
70. Kenyon K, Ousler GW, Watson M, et al. Efficacy and safety of the melanocortin agonist PL9643 in a phase 2 study of subjects with dry eye disease. Invest Ophthalmol Visual Sci. 2021;3:1.
71. A phase 3, multi-center study evaluating PL9643 in patients with dry eye (MELODY-1). NCT05201170. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05201170. Accessed July 19, 2024.
72. Kinoshita S, Awamura S, Nakamichi N, et al. A multicenter, open-label, 52-week study of 2% rebamipide (OPC-12759) ophthalmic suspension in patients with dry eye. Am J Ophthalmol. 2014;157(3):576–83e1. doi:10.1016/j.ajo.2013.11.010
73. Study of rebamipide eye drops to treat dry eye. NCT00201981. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT00201981?term=NCT00201981&rank=1.
74. Study of rebamipide eye drops to treat dry eye. NCT00201955. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT00201955?term=NCT00201955&rank=1.
75. Efficacy and safety of rebamipide in subjects with dry eye syndrome. NCT01632137. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT01632137?term=NCT01632137&rank=1.
76. Long term administration study of OPC-12759 ophthalmic suspension. NCT00818324. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT00818324?term=NCT00818324&rank=1.
77. Yoo H, Yoon S, Jang IJ, et al. Safety, tolerability, and serum/tear pharmacokinetics of human recombinant epidermal growth factor eyedrops in healthy subjects. Pharmaceuticals. 2022;15(11). doi:10.3390/ph15111312
78. Pharmacokinetics, safety, and tolerability of rhEGF eye drops in healthy male subjects. NCT05219461. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05219461?term=NCT05219461&rank=1.
79. Sacchetti M, Lambiase A, Schmidl D, et al. Effect of recombinant human nerve growth factor eye drops in patients with dry eye: a phase IIa, open label, multiple-dose study. Br J Ophthalmol. 2020;104(1):127–135. doi:10.1136/bjophthalmol-2018-312470
80. A study to evaluate safety and efficacy of rhNGF eye solution vs vehicle in patients with moderate to severe dry eye. NCT03982368. Clinical Trials.gov. Available from: https://clinicaltrials.gov/search?term=NCT03982368.
81. Clark D, Sheppard J, Brady TC. A randomized double-masked phase 2a trial to evaluate activity and safety of topical ocular reproxalap, a novel RASP inhibitor, in dry eye disease. J Ocul Pharmacol Ther. 2021;37(4):193–199. doi:10.1089/jop.2020.0087
82. A multi-center, double-masked, randomized, vehicle-controlled, parallel-group clinical trial evaluating the safety of reproxalap ophthalmic solution in subjects with dry eye disease. NCT04735393. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04735393?term=NCT04735393&rank=1.
83. The TRANQUILITY trial: clinical trial to assess the efficacy and safety in subjects with dry eye disease. NCT04674358. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04674358?term=%20NCT04674358&rank=1.
84. Beining MW, Magno MS, Moschowits E, et al. In-office thermal systems for the treatment of dry eye disease. Surv Ophthalmol. 2022;67(5):1405–1418. doi:10.1016/j.survophthal.2022.02.007
85. Vehicle-controlled study of SkQ1 as treatment for dry-eye syndrome (Vista-2). NCT04206020. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04206020?term=NCT04206020&rank=1.
86. Study of SkQ1 as treatment for dry-eye syndrome (Vista-1). NCT03764735. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT03764735?term=NCT03764735&rank=1.
87. Dong Y, Wang S, Cong L, et al. TNF-alpha inhibitor tanfanercept (HBM9036) improves signs and symptoms of dry eye in a phase 2 trial in the controlled adverse environment in China. Int Ophthalmol. 2022;42(8):2459–2472. doi:10.1007/s10792-022-02245-1
88. A study to assess the efficacy and safety of tanfanercept (HL036) ophthalmic solution in participants with dry eye (VELOS-3). NCT05109702. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05109702?term=NCT05109702&rank=1.
89. A study to assess efficacy and safety of HL036 in subjects with dry eyes (VELOS-2). NCT03846453. ClinicalTrial.gov. Available from: https://clinicaltrials.gov/study/NCT03846453?term=NCT04498182&cond=NCT03846453&rank=1.
90. Chen GL, Lei M, Zhou LP, Zeng B, Zou F. Borneol is a TRPM8 agonist that increases ocular surface wetness. PLoS One. 2016;11(7):e0158868. doi:10.1371/journal.pone.0158868
91. Fakih D, Baudouin C, Reaux-Le Goazigo A, Melik Parsadaniantz S. TRPM8: a therapeutic target for neuroinflammatory symptoms induced by severe dry eye disease. Int J Mol Sci. 2020;21(22). doi:10.3390/ijms21228756
92. Wirta DL, Senchyna M, Lewis AE, et al. A randomized, vehicle-controlled, phase 2b study of two concentrations of the TRPM8 receptor agonist AR-15512 in the treatment of dry eye disease (COMET-1). Ocul Surf. 2022;26:166–173. doi:10.1016/j.jtos.2022.08.003
93. Messmer EM. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch Arztebl Int. 2015;112(5):71–81;quiz82. doi:10.3238/arztebl.2015.0071
94. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15(3):511–538. doi:10.1016/j.jtos.2017.05.004
95. Kshirsagar NA, Munshi R, Bavdekar SB, Saxena R. Irrational ophthalmic fixed-dose combinations for dry eye syndrome. Indian J Ophthalmol. 2022;70(10):3687–3689. doi:10.4103/ijo.IJO_1169_22
96. Vazirani J, Sridhar U, Gokhale N, Doddigarla VR, Sharma S, Basu S. Autologous serum eye drops in dry eye disease: preferred practice pattern guidelines. Indian J Ophthalmol. 2023;71(4):1357–1363. doi:10.4103/IJO.IJO_2756_22
97. Razeghinejad MR, Katz LJ. Steroid-induced iatrogenic glaucoma. Ophthalmic Res. 2012;47(2):66–80. doi:10.1159/000328630
98. Kawabe A, Uesawa Y. Analysis of corticosteroid-induced glaucoma using the Japanese adverse drug event reporting database. Pharmaceuticals. 2023;16(7). doi:10.3390/ph16070948
99. Marsh P, Pflugfelder SC. Topical nonpreserved methylprednisolone therapy for keratoconjunctivitis sicca in Sjogren syndrome. Ophthalmology. 1999;106(4):811–816. doi:10.1016/S0161-6420(99)90171-9
100. Alcon Laboratories, Inc. EYSUVIS (Loteprednol Etabonate Ophthalmic Suspension) [Product Insert] 0.25%, for Topical Ophthalmic Use. Fort Worth, TX: Alcon Laboratories, Inc; 2020.
101. Alcon to acquire EYSUVIS adding to its ophthalmic eye drop portfolio. Available from: https://s1.q4cdn.com/963204942/files/doc_news/2022/05/Kala_News-Release-_FINAL-(1).pdf.
102. Venkateswaran N, Bian Y, Gupta PK. Practical guidance for the use of loteprednol etabonate ophthalmic suspension 0.25% in the management of dry eye disease. Clin Ophthalmol. 2022;16:349–355. doi:10.2147/OPTH.S323301
103. Comstock TL, Decory HH. Advances in corticosteroid therapy for ocular inflammation: loteprednol etabonate. Int J Inflam. 2012;2012:789623. doi:10.1155/2012/789623
104. Scottish Medicines Consortium. Verkazia (ciclosporin) 1mg/mL (0.1%) eye drops emulsion. Healthcare Improvement Scotland. Available from: https://www.scottishmedicines.org.uk/media/3957/ciclosporin-verkazia-final-nov-2018-for-website.pdf.
105. Bausch & Lomb Americas Inc. MIEBO (Perfluorohexyloctane Ophthalmic Solution), for Topical Ophthalmic Use. Bridgewater, NJ: Bausch & Lomb Americas Inc; 2023.
106. Mallinckrodt ARD LLC. ACTHAR GEL (Repository Corticotropin Injection) [Product Insert], for Intramuscular or Subcutaneous Use. Bedminster, NJ: Mallinckrodt ARD LLC; 2021.
107. Tapia C, Nessel TA, Zito PM. Cyclosporine. Treasure Island, FL: StatPearls Publishing; 2023.
108. Mouzaki A, Dai Y, Weil R, Rungger D. Cyclosporin A and FK506 prevent the depression of the IL-2 gene in mitogen-induced primary T lymphocytes. Cytokine. 1992;4(2):151–160. doi:10.1016/1043-4666(92)90050-2
109. Novaliq announces FDA approval of VEVYE™ (cyclosporine ophthalmic solution) 0.1%, for the treatment of the signs and symptoms of dry eye disease. Available from: https://www.novaliq.com/press-releases/2023/06/08/novaliq-announces-fda-approval-of-vevye-cyclosporine-ophthalmic-solution-0-1-for-The-treatment-of-The-signs-and-symptoms-of-dry-eye-disease/.
110. FDA approves generic version of cyclosporine ophthalmic emulsion as dry eye treatment. Available from: https://www.ophthalmologytimes.com/view/fda-approves-generic-version-of-cyclosporine-ophthalmic-emulsion-as-dry-eye-treatment.
111. Restasis cyclosporine ophthalmic emulsion. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2003/21-023_Restasis.cfm#:~:text=Approval%20Date%3A%2010%2F10%2F2003.
112. Agarwal P, Rupenthal ID. Non-aqueous formulations in topical ocular drug delivery - A paradigm shift? Adv Drug Deliv Rev. 2023;198:114867. doi:10.1016/j.addr.2023.114867
113. Gao D, Da Z, Yang K, Shi Y. Comparison of seven cyclosporine A formulations for dry eye disease: a systematic review and network meta-analysis. Front Pharmacol. 2022;13:882803. doi:10.3389/fphar.2022.882803
114. Chung JK, Spencer E, Hunt M, McCauley T, Welty D. Ocular distribution and pharmacokinetics of lifitegrast in pigmented rabbits and mass balance in beagle dogs. J Ocul Pharmacol Ther. 2018;34(1–2):224–232. doi:10.1089/jop.2017.0106
115. Nichols KK, Donnenfeld ED, Karpecki PM, et al. Safety and tolerability of lifitegrast ophthalmic solution 5.0%: pooled analysis of five randomized controlled trials in dry eye disease. Eur J Ophthalmol. 2019;29(4):394–401. doi:10.1177/1120672118791936
116. Nichols KK, Holland E, Toyos MM, et al. Ocular comfort assessment of lifitegrast ophthalmic solution 5.0% in OPUS-3, a phase III randomized controlled trial. Clin Ophthalmol. 2018;12:263–270. doi:10.2147/OPTH.S152841
117. Donnenfeld ED, Karpecki PM, Majmudar PA, et al. Safety of lifitegrast ophthalmic solution 5.0% in patients with dry eye disease: a 1-year, multicenter, randomized, placebo-controlled study. Cornea. 2016;35(6):741–748. doi:10.1097/ICO.0000000000000803
118. Frampton JE. Varenicline solution nasal spray: a review in dry eye disease. Drugs. 2022;82(14):1481–1488. doi:10.1007/s40265-022-01782-4
119. Quiroz-Mercado H, Hernandez-Quintela E, Chiu KH, Henry E, Nau JA. A phase II randomized trial to evaluate the long-term (12-week) efficacy and safety of OC-01 (varenicline solution) nasal spray for dry eye disease: the MYSTIC study. Ocul Surf. 2022;24:15–21. doi:10.1016/j.jtos.2021.12.007
120. Wirta D, Vollmer P, Paauw J, et al. Efficacy and safety of OC-01 (varenicline solution) nasal spray on signs and symptoms of dry eye disease: the ONSET-2 phase 3 randomized trial. Ophthalmology. 2022;129(4):379–387. doi:10.1016/j.ophtha.2021.11.004
121. Maisto R, Gesualdo C, Trotta MC, et al. Melanocortin receptor agonists MCR(1-5) protect photoreceptors from high-glucose damage and restore antioxidant enzymes in primary retinal cell culture. J Cell Mol Med. 2017;21(5):968–974. doi:10.1111/jcmm.13036
122. Tauber J, Berdy GJ, Wirta DL, Krosser S, Vittitow JL, Group GS. NOV03 for dry eye disease associated with meibomian gland dysfunction: results of the randomized phase 3 GOBI study. Ophthalmology. 2023;130(5):516–524. doi:10.1016/j.ophtha.2022.12.021
123. Wang X, Fan Y, Lan H, et al. The efficacy and safety of acupuncture or combined with western medicine for dry eye: a protocol for systematic review and meta-analysis. Medicine. 2020;99(35):e21878. doi:10.1097/MD.0000000000021878
124. Kim TH, Kang JW, Kim KH, et al. Acupuncture for the treatment of dry eye: a multicenter randomised controlled trial with active comparison intervention (artificial teardrops). PLoS One. 2012;7(5):e36638. doi:10.1371/journal.pone.0036638
125. Ji MH, Moshfeghi DM, Periman L, et al. Novel extranasal tear stimulation: pivotal study results. Transl Vis Sci Technol. 2020;9(12):23. doi:10.1167/tvst.9.12.23
126. Vigo L, Pellegrini M, Carones F, Scorcia V, Giannaccare G. Short-term effects of a novel eye mask producing heat and vibration for the treatment of meibomian gland dysfunction: a pilot study. J Ophthalmol. 2021;2021:1370002. doi:10.1155/2021/1370002
127. Zhang-Nunes S, Guo S, Lee D, Chang J, Nguyen A. Safety and efficacy of an augmented intense pulse light protocol for dry eye syndrome and blepharitis. Photobiomodul Photomed Laser Surg. 2021;39(3):178–184. doi:10.1089/photob.2020.4913
128. Sim HS, Petznick A, Barbier S, et al. A randomized, controlled treatment trial of eyelid-warming therapies in meibomian gland dysfunction. Ophthalmol Ther. 2014;3(1–2):37–48. doi:10.1007/s40123-014-0025-8
129. Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomed Laser Surg. 2015;33(1):41–46. doi:10.1089/pho.2014.3819
130. El Shami M, Maroun A, Hoyek S, Antoun J. Optimized combined low level light therapy and intense pulsed light therapy for the treatment of dry eye syndrome caused by meibomian glands dysfunction. J Fr Ophtalmol. 2022;45(10):1126–1136. doi:10.1016/j.jfo.2022.03.015
131. Li S, Yang K, Wang J, et al. Effect of a novel thermostatic device on meibomian gland dysfunction: a randomized controlled trial in Chinese patients. Ophthalmol Ther. 2022;11(1):261–270. doi:10.1007/s40123-021-00431-5
132. Trivli A, Karmiris E, Dalianis G, Ruggeri A, Terzidou C. Evaluating the efficacy of Quantum Molecular Resonance (QMR) electrotherapy in mixed-type dry eye patients. J Optom. 2023;16(2):128–134. doi:10.1016/j.optom.2022.06.003
133. Karpecki PM, Weiss SL, Kramer WG, et al. A phase 1, open-label, single-arm study evaluating the ocular safety of OTX-101 and systemic absorption of cyclosporine in healthy human volunteers. Clin Ophthalmol. 2019;13:591–596. doi:10.2147/OPTH.S187945
134. Giannaccare G, Taroni L, Senni C, Scorcia V. Intense pulsed light therapy in the treatment of meibomian gland dysfunction: current perspectives. Clin Optom. 2019;11:113–126. doi:10.2147/OPTO.S217639
135. Toyos R, Desai NR, Toyos M, Dell SJ. Intense pulsed light improves signs and symptoms of dry eye disease due to meibomian gland dysfunction: a randomized controlled study. PLoS One. 2022;17(6):e0270268. doi:10.1371/journal.pone.0270268
136. Marques JH, Baptista PM, Almeida D, José D, Sousa PJM, Barbosa I. Low-level light therapy in association with intense pulsed light for meibomian gland dysfunction. Clin Ophthalmol. 2022;16:4003–4010 doi:10.2147/OPTH.S384360.
137. Park Y, Kim H, Kim S, Cho KJ. Effect of low-level light therapy in patients with dry eye: a prospective, randomized, observer-masked trial. Sci Rep. 2022;12(1):3575. doi:10.1038/s41598-022-07427-6
138. Tai MC, Cosar CB, Cohen EJ, Rapuano CJ, Laibson PR. The clinical efficacy of silicone punctal plug therapy. Cornea. 2002;21(2):135–139. doi:10.1097/00003226-200203000-00001
139. Pellegrini M, Bernabei F, Moscardelli F, et al. Assessment of corneal fluorescein staining in different dry eye subtypes using digital image analysis. Transl Vis Sci Technol. 2019;8(6):34. doi:10.1167/tvst.8.6.34
140. Vigo L, Senni C, Pellegrini M, et al. Effects of a new formulation of multiple-action tear substitute on objective ocular surface parameters and ocular discomfort symptoms in patients with dry eye disease. Ophthalmol Ther. 2022;11(4):1441–1447. doi:10.1007/s40123-022-00518-7
141. Bilstein A, Heinrich A, Rybachuk A, Mosges R. Ectoine in the treatment of irritations and inflammations of the eye surface. Biomed Res Int. 2021;2021:8885032. doi:10.1155/2021/8885032
142. Chen W, Zhang X, Liu M, et al. Trehalose protects against ocular surface disorders in experimental murine dry eye through suppression of apoptosis. Exp Eye Res. 2009;89(3):311–318. doi:10.1016/j.exer.2009.03.015
143. Efficacy and safety study of HU00701/HU007 eye drops in patients with dry eye syndrome. NCT03461575. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT03461575. Accessed October 3, 2023.
144. Gupta PK, Periman LM, Lain E, et al. Meibomian gland dysfunction: a dermatological perspective on pathogenesis and treatment outlook. Clin Ophthalmol. 2021;15:4399–4404. doi:10.2147/OPTH.S327407
145. Rao K, Farley WJ, Pflugfelder SC. Association between high tear epidermal growth factor levels and corneal subepithelial fibrosis in dry eye conditions. Invest Ophthalmol Vis Sci. 2010;51(2):844–849. doi:10.1167/iovs.09-3875
146. Swartz W. Reproxalap for the treatment of dry eye disease. Touch Rev Ophthalmol. 2023;17(1):31–35. doi:10.17925/USOR.2023.17.1.31
147. Na JY, Huh KY, Yu KS, et al. Safety, tolerability, and pharmacokinetics of single and multiple topical ophthalmic administration of imatinib mesylate in healthy subjects. Clin Transl Sci. 2022;15(5):1123–1130. doi:10.1111/cts.13226
148. Evans D, Kenyon K, Ousler G, et al. Efficacy and safety of the melanocortin pan-agonist PL9643 in a phase 2 study of patients with dry eye disease. J Ocul Pharmacol Ther. 2023;39(9):600–610. doi:10.1089/jop.2023.0056
149. Bui HL, Su YH, Yang CJ, Huang CJ, Lai JY. Mucoadhesive, antioxidant, and lubricant catechol-functionalized poly(phosphobetaine) as biomaterial nanotherapeutics for treating ocular dryness. J Nanobiotechnology. 2024;22(1):160. doi:10.1186/s12951-024-02448-x
150. Joshi VP, Singh S, Thacker M, et al. Newer approaches to dry eye therapy: nanotechnology, regenerative medicine, and tissue engineering. Indian J Ophthalmol. 2023;71(4):1292–1303. doi:10.4103/IJO.IJO_2806_22
151. Yang CJ, Anand A, Huang CC, Lai JY. Unveiling the power of gabapentin-loaded nanoceria with multiple therapeutic capabilities for the treatment of dry eye disease. ACS Nano. 2023;17(24):25118–25135. doi:10.1021/acsnano.3c07817
152. Fromstein SR, Harthan JS, Patel J, Opitz DL. Demodex blepharitis: clinical perspectives. Clin Optom. 2018;10:57–63. doi:10.2147/OPTO.S142708
153. Choi Y, Eom Y, Yoon EG, Song JS, Kim IH, Kim HM. Efficacy of topical ivermectin 1% in the treatment of demodex blepharitis. Cornea. 2022;41(4):427–434. doi:10.1097/ICO.0000000000002802
154. Yeu E, Wirta DL, Karpecki P, Baba SN, Holdbrook M, Saturn ISG. Lotilaner ophthalmic solution, 0.25%, for the treatment of demodex blepharitis: results of a prospective, randomized, vehicle-controlled, double-masked, pivotal trial (Saturn-1). Cornea. 2023;42(4):435–443. doi:10.1097/ICO.0000000000003097
155. Frame K, Cheung IMY, Wang MTM, Turnbull PR, Watters GA, Craig JP. Comparing the in vitro effects of MGO™ manuka honey and tea tree oil on ocular demodex viability. Cont Lens Anterior Eye. 2018;41(6):527–530. doi:10.1016/j.clae.2018.06.006
156. Cheng SN, Jiang FG, Chen H, Gao H, Huang YK. Intense pulsed light therapy for patients with meibomian gland dysfunction and ocular demodex infestation. Curr Med Sci. 2019;39(5):800–809. doi:10.1007/s11596-019-2108-1
157. Tarsus Pharmaceuticals, Inc. XDEMVY™ (Lotilaner Ophthalmic Solution) [Product Insert] 0.25%, for Topical Ophthalmic Use. Irvine, CA: Tarsus Pharmaceuticals, Inc; 2023.
158. Trattler W, Karpecki P, Rapoport Y, et al. The prevalence of demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign. Clin Ophthalmol. 2022;16:1153–1164. doi:10.2147/OPTH.S354692
159. Messmer EM, Ahmad S, Benitez Del Castillo JM, et al. Management of inflammation in dry eye disease: recommendations from a European panel of experts. Eur J Ophthalmol. 2022:11206721221141481. doi:10.1177/11206721221141481
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.