")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Diagnosing and Discussing Sexual Abuse: A Scoping Review on Training Methods for Health Care Professionals
Authors van Zyl-Bonk FE , Lange S, Lagro-Janssen ALM , Teunissen TAM
Received 2 November 2023
Accepted for publication 4 March 2024
Published 27 March 2024 Volume 2024:15 Pages 243—255
DOI https://doi.org/10.2147/AMEP.S444718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Fiona Elizabeth van Zyl-Bonk, Sibylle Lange, Antoinette Leonarda Maria Lagro-Janssen, Theodora Alberta Maria Teunissen
Department of Primary and Community Care, Research Institute for Medical Innovation, Radboud University Medical Center, Nijmegen, the Netherlands
Correspondence: Theodora Alberta Maria Teunissen, Department of Primary and Community Care, Research Institute for Medical Innovation, Radboud University Medical Center, Geert Grooteplein 21, Postbus 9101, Nijmegen, 6500 HB, the Netherlands, Tel +31 24 3618181, Email [email protected]
Purpose: Sexual abuse is a health issue with many consequences. Recognizing and discussing past sexual abuse has proven to be challenging for health care professionals. To improve overall quality of health care for sexual abuse victims, health care professionals need to be properly trained. The aim of this paper is to provide an overview of training methods for health care professionals and to report on their effectiveness.
Methods: A scoping review was conducted. A broad search was executed in six databases in December 2022. Study selection was performed by two independent reviewers, followed by quality assessment and data extraction.
Results: After screening of titles and abstracts and later full-text assessment for quality appraisal, seven articles were selected, consisting mostly of non-randomized trials, performed among a total of 1299 health care professionals. All studies were assessed to be of moderate to poor quality. The participants attended training courses with a wide variety of durations, settings, formats and methods. The outcomes showed improvements in self-perceived or measured knowledge, skills and confidence to discuss sexual violence. Changes in clinical practice were scarcely investigated. Training courses were most effective when a mix of didactic passive methods, such as lectures and videos, and active participatory strategies, such as discussions and roleplay, were applied. Timely iteration to reinforce retention of gained knowledge and skills also contributed to effectiveness. Participants most enjoyed incorporating opportunities for receiving feedback in small settings and sharing personal experiences.
Conclusion: This scoping review summarizes on how to effectively train health care professionals. Flaws and difficulties in measuring the effectiveness of training courses were discussed. Recognition and discussion of past sexual abuse by health care providers can be effectively trained using an alternating mix of multiple active and passive training methods with room for feedback and personal experiences.
Keywords: sexual violence, disclosure, recognition, medical education, post-graduate training
Introduction
Sexual abuse (SA) is a broad term describing all forms of sexual contact or behaviour without consent. More than 40% of women and nearly 25% of men have experienced some form of sexual violence in their lifetime.1–3 Trauma, including sexual violence, is highly stressful and causes activation of the Hypothalamic-Pituitary-Adrenal (HPA) axis which initiates the interaction between cortisol and the immune system. Stress initially results in increased levels of cortisol. When stress is too high and persists for too long, the HPA axis becomes dysfunctional and may be related to several diseases. Dysregulation of the immune system is a known cause of autoimmune- and chronic diseases such as cardiovascular diseases, chronic pain syndromes and asthma.4 With a quarter of victims experiencing short- and long-term physical, psychological, relational and/or sexual consequences, the acute and chronic health issues of SA victims are extensive.2
Only eight per cent of victims disclose to professional care, mostly to general practitioners, psychologists and social workers.2
Victims experience several barriers to disclosure that are also associated with post-traumatic stress, such as avoidance of painful memories, shame and inexpressibility. The fear of not being believed, of being blamed and of facing possible post-disclosure consequences are often reasons for victims to withhold their past SA.5–10 Most importantly, patients themselves often fail to recognize the relation between a history of sexual trauma and their current physical or mental symptoms.7
HCPs in their turn do not sufficiently recognize or respond to a possible history of SA in their patients either, which is mostly due to lack of knowledge or to personal barriers. HCPs are often ignorant of SA indicators, lack a consistent approach in addressing suspected abuse and do not know where to refer patients for further treatment after disclosure.11–13 Personal barriers include HCPs not feeling comfortable addressing this subject, not having enough time to engage with it during consultations and the commonly held misconception that they are not the right person to disclose to because they believe SA is not a medical problem.11,12,14 HCPs also mention that asking about SA can be too invasive and distressing for patients, as it could open up “Pandora’s box”.11,15,16 In contrast with these self-imposed feelings in HCPs, patients say they consider questions about past SA by HCPs as legitimate and appropriate.9 When patients are explicitly asked about negative sexual experiences, disclosures increased by 25% compared to when they were not asked.16,17
When HCPs lack the competencies to identify and discuss sexual trauma in a correct way, they potentially fail to provide appropriate care to sexually abused patients. It is also important because health care settings can easily trigger sexually traumatized patients, which may lead to further revictimization and re-traumatization as health care givers do not always respond respectfully and with recognition of the trauma when a patient discloses sexual abuse. This can (unintentionally) give a victim the impression that she/he is to blame. Also physical examinations can trigger victims because of the physical contact, especially a gynecological examination.3,4
Appropriately trained HCPs, however, can help to alleviate the health consequences of sexual violence and even reduce its recurrence.18 Studies on training methods geared towards recognizing and discussing intimate partner violence, a closely related subject, have seen successful results.16,19 Little research has been done, however, on training methods regarding recognizing and discussing SA.12,20
In order to provide a concise overview of how to properly train HCPs, we conducted a scoping review addressing the following question: what training methods are there for health care providers to improve on recognizing and discussing sexual trauma in adult patients, and what is their effectiveness? The aims of this scoping review were: to (1) conduct a systematic search of published literature on training methods for health care providers on recognizing and discussing past SA in adult patients; (2) map out the characteristics and range of methodologies used in these training methods; (3) report on whether and how these training methods improve recognition and discussion of sexual abuse; and (4) propose recommendations for the future development of training curricula dealing with this subject.
Materials and Methods
Protocol
The methodology of this scoping review was based on the framework outlined by Arksey and O’Malley (2005) and guided by the PRISMA extension for scoping reviews (PRISMA-ScR).21,22
Data Sources and Search Strategy
The initial search was conducted on December 5, 2022, in six electronic databases: PubMed, EMBASE, PsycINFO, CINAHL, Cochrane and Web of Science. The search query was built using MeSH terms (Appendix 1) and free text terms (Appendix 2), focusing on a broad range of articles. The database search was limited to articles published in the languages “English” or “Dutch”. No further limits for date, study design or type were applied. After the search had been performed, studies were collected in data manager “EndNote 20.3” and deduplicated until no further duplicates were found. The articles were imported into data managing and data streaming software “Covidence” (Covidence.org), after which seven more duplicates were manually removed. No additional literature was found through forward and backward citation.
Eligibility Criteria
A two-stage screening process was used to assess the relevance of studies identified in the search. Studies needed to fit the following criteria to be eligible for inclusion: the article discussed a training course focusing on improving recognition and discussion of past sexual abuse presented by patients over 18 years of age; the training course was targeting HCPs and future HCPs; and the study was written in English or Dutch. Exclusion criteria were: training course focusing on improving recognition and discussion of SA in victims with intellectual or physical disabilities, victims of genital mutilation and victims of physical and psychological interpersonal violence other than sexual violence.
Study Selection Process and Critical Appraisal
For the first level of study selection, the articles were screened by one reviewer (SL) on title and abstract based on the inclusion and exclusion criteria. Titles (n=3) for which an abstract was not available were included for subsequent review of the full article in the data characterization phase. During the second phase of screening, all articles deemed relevant after title and abstract screening were procured for review of the full-text article. If articles could not be obtained through institutional holdings available to the authors, attempts were made to contact the source author or journal for assistance. The article was excluded if its full-text version proved to be irretrievable.
The characteristics of each full text were first independently extracted by two reviewers (SL, FZ), after which they met to discuss and resolve any conflicts. To help ensure consistency with the research question and purpose, the supervisor (TT) subjoined three times as a third party to resolve disagreements. The interobserver agreement was estimated as kappa 0.72 (95% CI [0.426–1.00], p<0.001).
Because the included studies were single-arm and randomized controlled trials, the MINORS checklist was chosen to assess the quality of the articles.23 To fit the feasibility of follow-up within this field of research, we decided to tailor item six on this checklist from a two-year into two-month follow-up. The reviewers (SL, FZ, TT) independently assessed an included article as a try-out, after which the quality assessment was discussed to ensure equal interpretation of the MINORS checklist. After pilot-testing, the quality of all articles was independently and blindly assessed by the two reviewers (SL, FZ).
Data Characterization and Synthesis
To determine which variables to extract (Appendix 3), a simplified data-charting template was developed by the team based on the JBI Reviewers Manual, and this template was inserted in Covidence.24 Two reviewers (SL, FZ) first independently charted the data before coming together to discuss and merge their findings. The data were extracted from Covidence and compiled in Microsoft Excel 2016.
Results
Search and Selection of Studies
The database search conducted in December 2022 yielded 13,656 studies, 8897 of which remained after automatic and manual deduplication. After screening of title and abstract, 33 of these studies were considered potentially relevant. After full text assessment, 26 articles were excluded for discussing a topic or targeting a population that did not meet our inclusion criteria. Finally, a total of seven studies were selected that did meet the inclusion criteria. The flow of articles from identification to final inclusion is represented in Figure 1.
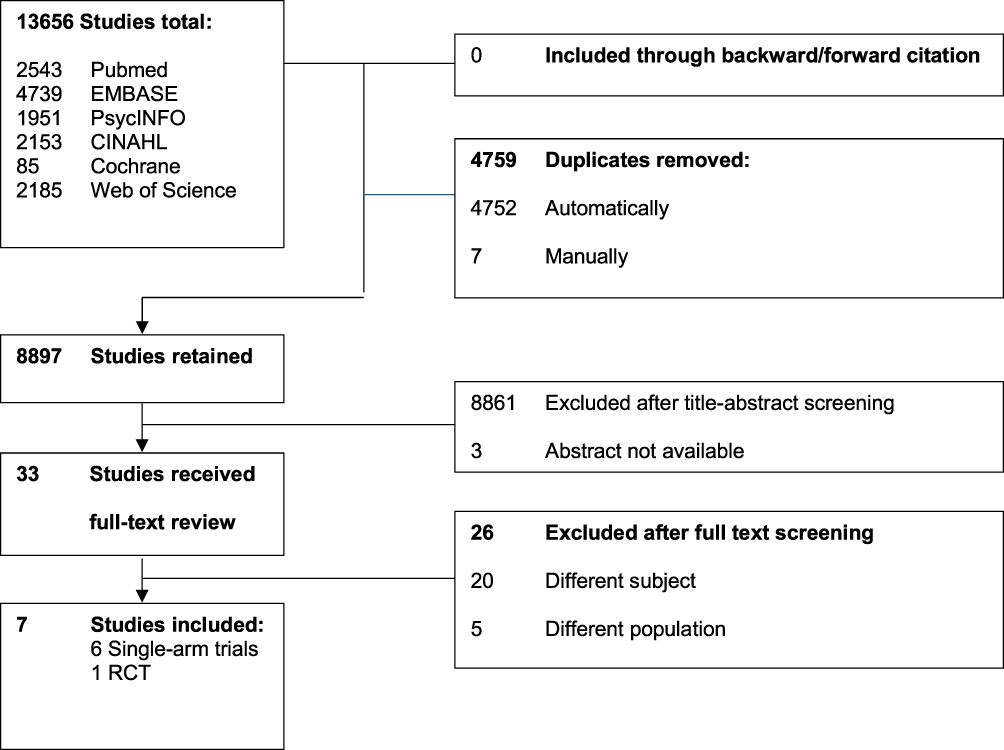 |
Figure 1 Flowchart of literature search and study selection process. |
General Characteristics and Quality Appraisal
The general characteristics of articles included in this study are reported in Table 1. All studies were published between 1990 and 2021.25–31 The majority of studies were conducted in North America (United States and Canada), and the remaining two studies were conducted in Europe (Ireland) and in Oceania (New Zealand). Six studies used a pre- and post-test questionnaire, and two studies also followed up a third time after several weeks to several months. Six studies were single-arm non-randomized controlled trials (NRS), and one study was a multi-arm randomized controlled trial (RCT). According to the MINORS checklist (Figure 2), all studies were assessed as being of moderate to poor quality.
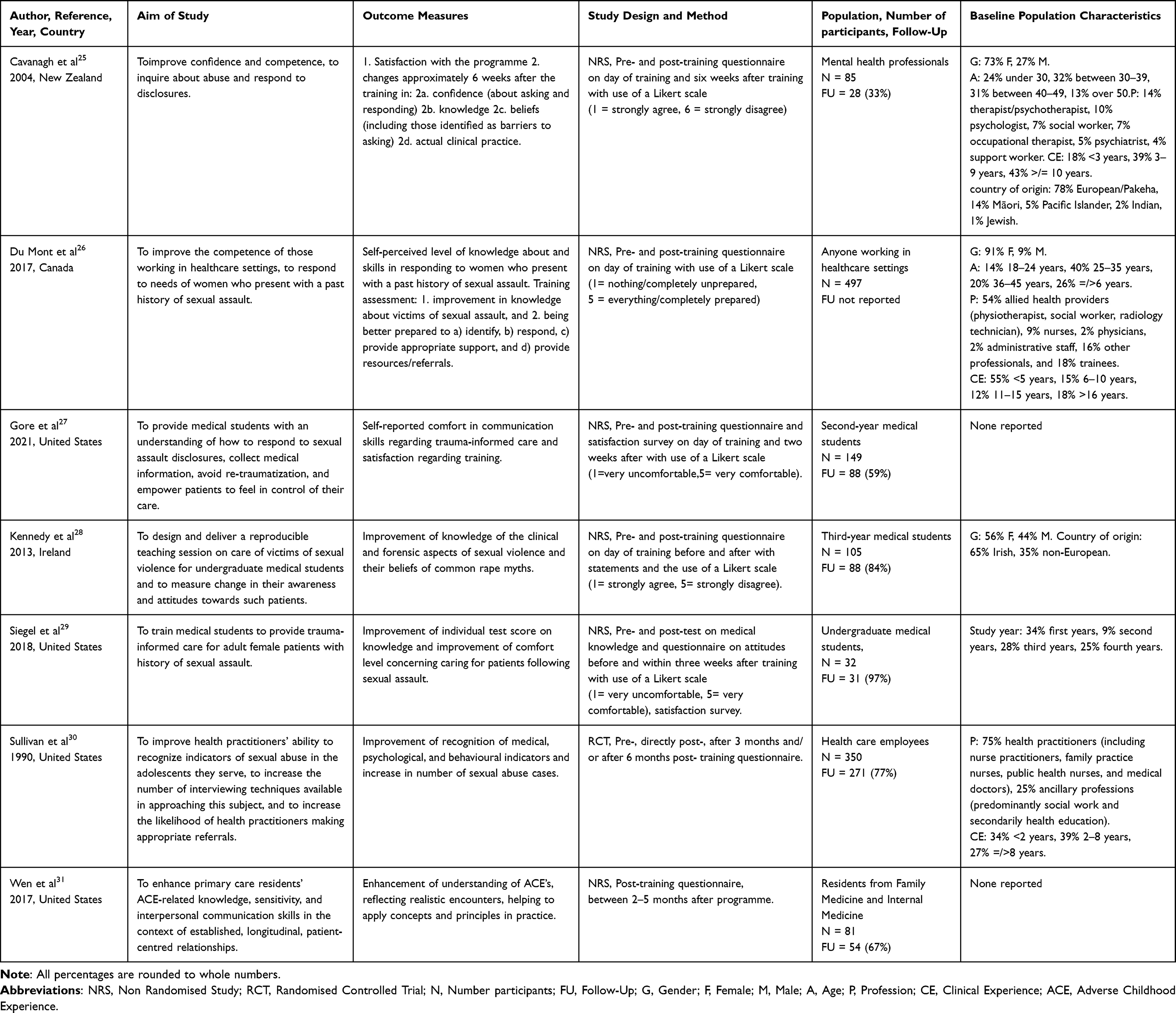 |
Table 1 General Study Characteristics in Alphabetical Order Authors |
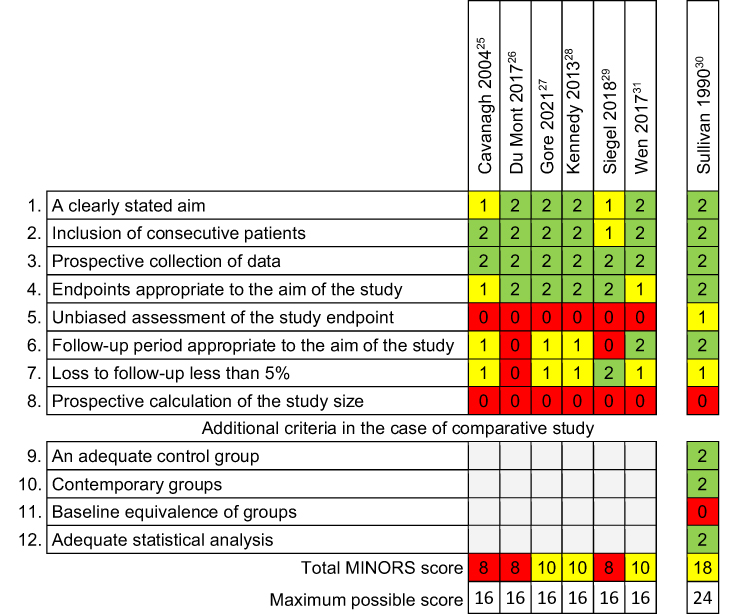 |
Figure 2 Quality Assessment of selected articles with the MINORS checklist. The items are scored 0 (not reported), 1 (reported but inadequate) or 2 (reported and inadequate). Red = poor quality, yellow = moderate quality, green = good quality. The global ideal score being 16 for non-comparative studies and 24 for comparative studies. |
Characteristics of Participants
This scoping review included a total of 1299 (future) health care professionals, with Cavanagh (N=85), Siegel (N=32) and Wen (N=81) all having study samples of less than 100 participants. Six articles mentioned numbers lost to follow-up. Siegel had 3% loss of follow-up; Kennedy had 16% loss of follow-up; and the other articles had >20% loss of follow-up. The 1299 participants consisted of 1013 (78.0%) HCPs and 286 (22.0%) medical students. The former group consisted of 472 (46.6%) clinically working HCPs and 540 (53.4%) allied HCPs, with one study including only mental health professionals and another only family and internal medicine residents. Three studies mentioned the participants’ gender, which showed a female predominance of 573 (83.4%) female versus 114 (16.6%) male participants.
Characteristics of Interventions
The duration of interventions varied from one hour to one day, with Du Mont and Siegel having the shortest (one hour), and Cavanagh and Sullivan having the longest intervention (one day). Most studies utilized both didactic and participatory forms of conveying information during their training course. Didactic methods could consist of lectures, summaries, handouts, videos and/or audios. Participatory strategies could consist of scenarios or vignettes, discussions, specific exercises, simulation and/or roleplay. Siegel applied only didactic video and audio formats online. Kennedy’s intervention incorporated some form of interaction suggesting a participatory element, although this was not specified any further. All other studies used an alternating mix of multiple active and passive training methods.
Characteristics of Outcome Measures
The studies assessed a wide variety of outcome measures with some overlap in between. Kennedy focused almost entirely on changing beliefs and attitudes in students, by asking them whether they would agree with statements such as “women who wear certain types of clothing are responsible for being raped”. Cavanagh included common misconceptions among mental health professionals that may act as barriers to discussing SA, such as fear of offending or distressing patients. Whereas Du Mont measured the self-perceived level of certain skills, such as how to respond and provide adequate support and resources for referral, Sullivan assessed the actual skill of identifying indicators of SA. Both Kenney and Siegel measured knowledge of recognition of SA before and after the intervention through pre- and post-testing, whereas Du Mont measured self-perceived knowledge of SA before and after and Wen only after. Four studies evaluated changes in confidence and comfort in recognizing, discussing and responding to past SA. Two studies asked participants whether they expected a change in their clinical practice after the intervention, whereas Sullivan assessed actual change by asking participants to report on the number of victims identified after the intervention compared to before. Four studies also evaluated the training course itself.
Outcomes
The collection of outcomes can be found in Table 2. All included studies showed a statistically significant improvement on the outcome measures according to their aims. Siegel reported a significant increase of two more correctly answered knowledge-based questions in post-testing compared to pre-testing. Du Mont had an overall increase of 1.1 points on the 5-point Likert scale in increase of perceived knowledge of SA. In the study by Cavanagh, the number of mental health professionals who believed that SA disclosures were the result of psychotic delusions decreased by 2.7%. When rape myths were addressed, Kennedy showed a reduction of misconceptions about sexual violence (numbers not reported). Wen found that 65.6% (2014–2015) and 72.7% (2015–2016) of the participants agreed that the intervention helped to apply concepts and principles in practice, and 62.5% and 65.6% planned to implement these skills in their clinical practice. In the study by Cavanagh, HCPs experienced a 94% increase in confidence to inquire about and respond to SA. Du Mont showed that 96.4% of participants felt better prepared to identify and 96.8% to respond to SA. Students showed a significant change in self-reported comfort in communication skills in Gore (numbers not reported). In Siegel, comfort levels regarding care for sexually abused patients improved ranging from 19% to 27%. Three studies showed either participants’ change or expectation to change in their clinical practice after the intervention. In Cavanagh, 67% of the participants agreed with the statement “The training session has changed my clinical practice”, and 33% reported behavioural changes in their clinical practice. In Sullivan, the number of HCPs who had dealt with at least one case in the last three months prior to training rose from 15% to 20% six months after the intervention.
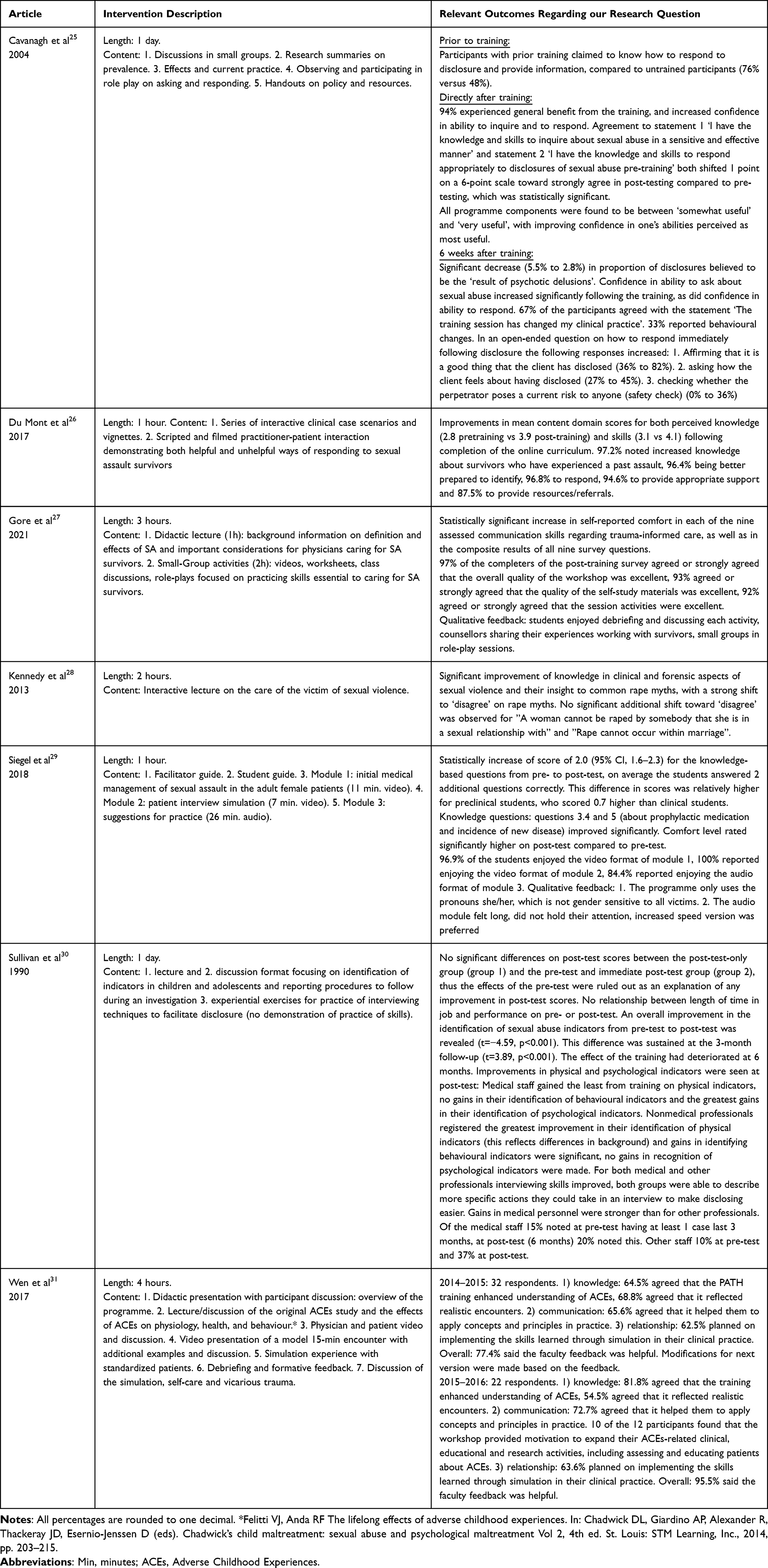 |
Table 2 Study Outcomes in Alphabetical Order Authors |
While post-training improvement on their defined outcome measures was universal for all studies, only one study evaluated whether this result could be maintained. Sullivan measured a significant improvement of identification of SA indicators in the post-test, a sustained significant improvement after three-months of follow-up, but a slight deterioration of this improvement after six months (numbers not reported).
In the studies that also evaluated the intervention itself, the training course was judged by participants as being enjoyable, of excellent quality, useful and motivating for applying knowledge in practice. Online-only training was experienced as isolating, while an alternating mix of active and passive training methods was found to be stimulating. Participatory components of the training course that were enjoyed most, were those in small settings and those incorporating a form of feedback, such as role play, discussions and debriefing. Participants also appreciated it when those conducting the training course shared their personal experiences with SA victims. Video materials of model patients and simulations with standardized patients were found to resemble realistic encounters. In Siegel’s exclusively online format, video materials were preferred to audio-only materials as the latter were not able to hold attention for long enough. Other criticisms concerned the lack of gender diversity in the use of victim pronouns and the duration of the training course being too limited to cover all aspects of SA.
Discussion
In conclusion, our search yielded seven studies that addressed our intended subject, consisting mostly of non-randomized trials. All participants were either active or training to be active in health care and were subjected to training courses with a wide variety of durations, settings, formats and methods. Most training courses focused on increasing knowledge. The outcomes showed improvements in self-perceived or measured knowledge, skills, confidence in addressing SA or, if measured, a beneficial change in clinical practice. Some decline was measured as time passed by. If assessed, interventions were rated as useful to the participants when both participatory and didactic methods, an element of feedback and personal experience sharing were incorporated into the training course. On-line training was experienced as isolating.
Strengths and Limitations of Included Studies
The studies included in this review used a wide range of methodologies to measure the effect of their training course. However, not all endpoints hold the same validity. We question whether evaluating subjective outcomes such as changes in knowledge and skills through participants’ self-report, as was done in three studies, has value for measuring actual change in their own clinical setting. Although self-reports are more accessible and easier to measure, drawing conclusions from self-perception is open to biasing influences, even under anonymity.25 Measuring confidence is even more challenging in this respect. No correlation between self-perceived confidence and formally assessed performance has been found, making the outcome of “self-perceived improvement” of limited usefulness in translation to practice.32 The ability to demonstrate and perform in practice is a more reliable indicator that the newly acquired knowledge, skills and attitudes have actually been integrated.33
All articles used surveys as an instrument for investigating their endpoints. As surveys are an inexpensive and simple means for extracting information such as preferences, opinions or facts, they are a suitable and predictable way of analysing this type of intervention. However, one should take into account that, due to their optional character, surveys contain both selection and non-response biases.34,35 Likert scales are a popular instrument for measuring attitudes, beliefs and perceptions in surveys, which is also reflected in this review as five out of seven articles used one or multiple Likert scales. Their popularity, however, does not necessarily equate to its validity as a data collection method.36 Depending on how questions are formulated, Likert scales can carry potential for bias as respondents tend to tick the middle answers and avoid the end of the scale. Also because of information loss as opposed to qualitative interviews, which are able to prevent such loss of information but, on a great scale, are immensely time-consuming and do not offer the same quantitative outcomes as surveys.37
Only one study used a randomized controlled trial design (evidence level II), while the remaining studies were single-arm NRS providing a lower level of evidence (level III-3). All included studies were rated by the MINORS checklist as being of moderate to poor quality, which was mostly based on the lack of blind assessment of endpoints (statement five), the loss of follow-up of more than 5% (statement seven) and the lack of prospective calculation of study size (statement eight). Although blinding and the use of control groups can help minimize bias in the analysis, this is very difficult to achieve when studies are conducted in an educational setting. A more attainable way, therefore, is to conduct testing before the intervention as well as after, which was done in all studies except one. The same holds true for what the MINORS checklist considers an acceptable amount of loss to follow-up. Only one study maintained 97% participants during follow-up, and one study maintained 84%, but the rest lost over 20% of its participants during follow-up, which would normally be considered a threat to validity.38 However, due to the above-mentioned optional character of survey studies, some loss to follow-up is to be expected and should, therefore, be judged less severely in our opinion.
Strengths and Limitations of This Review
To our knowledge, no review of any kind has been performed on training methods about SA, making this review the first to enhance our knowledge of training methods for HCPs to improve recognizing and discussing SA. Another strength of this scoping review is its use of guidance by validated PRISMA-ScR protocol and its supervisors with expertise on SA as well as on educational science. Transparency in the review process was provided. A broad scope was ensured by performing an extensive search using six search engines. The number and heterogeneity of the included articles showed that conducting a scoping review on the subject matter was the correct format. Because the applied training methods were so diverse, the subject could be evaluated from different angles, offering insight into a variety of training methods. For obvious reasons, assessments of the different interventions could not be compared, leaving room for future research to establish what duration, setting, format or method is preferred. Lastly, the scoping review was conducted independently by two researchers and intensively guided by two expert supervisors, confirming the validity of the outcomes.
Recommendations for Practice
Teaching HCPs to identify and respond to SA victims takes more than the mere transfer of knowledge. As Miller pointed out, what is needed to accomplish measurable change in practice is to know how to use the knowledge that has been acquired and to develop the skills to interpret and apply such knowledge.32 As a more intricate skillset is required, training courses using only didactic, or passive, learning techniques will have limited effect on changing practice. Based on the studies we compiled in this review, we recommend the use of mixed intervention methods, consisting of both didactic and participatory elements. Active learning techniques, also known as experiential learning, are said to increase engagement and motivation in students and are particularly important in the acquisition of skills. Though not impossible, experiential learning is hard to accomplish in a setting that is strictly online. Online-only training does not have the same benefits as classic face-to-face learning, is said to have isolating effects and can hamper the quality of discussion and debriefing.29,39 This is a challenge as online courses are more easily accessible to HCPs, and more and more postgraduate medical education courses are being offered online. That said, we propose that a training course on improving recognition and discussion of SA is not done online exclusively but at least partly in a live setting.
Role-play as part of active learning, as was used in three studies, is a training method that is well-known to medical education for practice and evaluation of skills. Using actors or scripts acted out by participants as standardized patients, role-play is a form of simulation that underlines the importance of the social context of learning. It is said to help participants gain better involvement, self-esteem and empathy as well as increased learning.40 It can also give more insight into their own as well as their patients’ feelings, which is especially helpful when it concerns a sensitive subject such as SA. In the studies we included, receiving feedback from educators on participatory exercises was particularly appreciated. Feedback during debriefing has been marked as the single most important feature of simulation-based education.41 To receive feedback has been shown to have motivational benefits for participants and to improve performance and speed in acquiring and applying knowledge.33 We suggest, therefore, that SA training for HCPs should involve a form of simulation or role-play that includes debriefing opportunities.
There was only one study that carried out a follow-up beyond five months and showed deterioration of skills six months after training.25 As it is a well-known fact that significant effects on health care knowledge are only achieved through repetition and reinforcement, this further confirms the need for reinforcement to maintain the impact of training courses.41 Consequently, a training course aiming to have lasting effects should also offer the possibility of a refresher course after six months.
It is vital to the enhancement of care to effectively train HCPs on how to diagnose and discuss a history of sexual abuse with patients. When developing new curricula for HCPs on this subject, training courses should employ alternating didactic and participatory learning methods and implement reinforcement within a time span of six months for sustainability. Training courses should preferably be face-to-face, showing how to apply knowledge and skills in practice, and their duration should be at least three hours to allow for transfer of knowledge and skills, feedback and role play practice to take place. With these insights, we hope to contribute to the further development of training courses aiming to equip health care professionals with better responses to the needs of victims of sexual abuse.
Conclusion
Most training courses for diagnosing and discussing sexual abuse for health care professionals focused on increasing knowledge. The outcomes showed improvements in self-perceived or measured knowledge, skills, confidence in addressing SA or, if measured, a beneficial change in clinical practice. If assessed, interventions were rated as useful to the participants when both participatory and didactic methods, an element of feedback and personal experience sharing were incorporated into the training course. On-line training was experienced as isolating. Recognition and discussion of past sexual abuse by health care providers can be effectively trained using an alternating mix of multiple active and passive training methods with room for feedback and personal experiences.
Abbreviations
HCPs, Health care professionals; NRS, Non-randomized study; RCT, Randomized controlled trial; SA, Sexual abuse.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Farahi N, McEachern M. Sexual assault of women. Am Fam Physician. 2021;103(3):168–176.
2. Akkersmans M, Gielen W, Kloosterman R, Moons E, Reep C, Wingen M. Prevalentiemonitor Huiselijk Geweld En Seksueel Geweld 2020. CBS, WODC; 2020.
3. Fergusson DM, McLeod GFH, Horwood LJ. Childhood sexual abuse and adult developmental outcomes: findings from a 30-year longitudinal study in New Zealand. Child Abuse Negl. 2013;37(9):664–674. doi:10.1016/j.chiabu.2013.03.013
4. Şimşek Ş, Kaplan İ, Uysal C, Yüksel T, Alaca R. The levels of cortisol, oxidative stress, and DNA damage in the victims of childhood sexual abuse: a Preliminary Study. J Child Sex Abus. 2016;25(2):175–184. doi:10.1080/10538712.2016.1123790
5. Nelson S, Baldwin N, Tatlor J. Mental health problems and medically unexplained physical symptoms in adult survivors of childhood sexual abuse: an integrative literature review. J Psychiatr Ment Health Nurs. 2012;19(3):211–220. doi:10.1111/j.1365-2850.2011.01772.x
6. Griffin VW, Wentz E, Meinert E. Explaining the why in #WhyIDidntReport: an examination of common barriers to formal disclosure of sexual assault in college students. J Interpers Violence. 2022;37(15–16):Np14716–np45. doi:10.1177/08862605211016343
7. Ullman SE, O’Callaghan E, Shepp V, Harris C. Reasons for and experiences of sexual assault nondisclosure in a diverse community sample. J Fam Violence. 2020;35(8):839–851. doi:10.1007/s10896-020-00141-9
8. Lomans AM, Uijen AA, Akkermans RP, Lagro-Janssen T, Teunissen DAM. Help-seeking behaviour in primary care of men and women with a history of abuse: a Dutch cohort study. Eur J Gen Pract. 2022;28(1):40–47. doi:10.1080/13814788.2022.2054985
9. Wendt EK, Lidell EA, Westerståhl AK, Marklund BR, Hildingh CI. Young women’s perceptions of being asked questions about sexuality and sexual abuse: a content analysis. Midwifery. 2011;27(2):250–256. doi:10.1016/j.midw.2009.06.008
10. Lagro-Janssen T. Waarom blijven slachtoffers van seksueel geweld verborgen? Huisarts Wet. 2022;65(11):24–9.11. doi:10.1007/s12445-022-1588-6
11. Leder MR, Emans SJ, Hafler JP, Rappaport LA. Addressing sexual abuse in the primary care setting. Pediatrics. 1999;104(2):270–275. doi:10.1542/peds.104.2.270
12. Weinreb L, Savageau JA, Candib LM, Reed GW, Fletcher KE, Hargraves JL. Screening for childhood trauma in adult primary care patients: a cross-sectional survey. Prim Care Compan J Clin Psychiatry. 2010;12(6). doi:10.4088/PCC.10m00950blu
13. Gruenfeld E, Willis DG, Easton SD. ”A very steep climb”: therapists’ perspectives on barriers to disclosure of child sexual abuse experiences for men. J Child Sex Abus. 2017;26(6):731–751. doi:10.1080/10538712.2017.1332704
14. Gerassi L, Pederson A. ‘Have you ever traded sex for money or drugs?’ Health care providers’ perspectives on sex trafficking risk assessments in clinics. J Health Ser Res Policy. 2021;26(4):272–281. doi:10.1177/1355819621997478
15. Lessing JE. Primary care provider interventions for the delayed disclosure of adolescent sexual assault. J Pediatr Health Care. 2005;19(1):17–24. doi:10.1016/S0891-5245(04)00181-6
16. Lo Fo Wong S. The doctor and the woman who ”fell down the stairs”. Family doctor’s role in recognising and responding to intimate partner abuse: [Sl: sn]; 2006.
17. Rickert VI, Edwards S, Harrykissoon SD, Wiemann CM. Violence in the lives of young women: clinical care and management. Curr Womens Health Rep. 2001;1(2):94–101.
18. Addressing violence against women in pre-service health training: integrating content from the Caring for women subjected to violence curriculum. WHO; 2022. Available from: https://www.who.int/publications/i/item/9789240064638.
19. Ambikile JS, Leshabari S, Ohnishi M. Curricular limitations and recommendations for training health care providers to respond to intimate partner violence: an integrative literature review. Trauma Violence Abuse. 2022;23(4):1262–1269. doi:10.1177/1524838021995951
20. Hart BJ, Klein A, editors. Practical implications of current intimate partner violence research for victim advocates and service providers; 2013.
21. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
22. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
23. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–716. doi:10.1046/j.1445-2197.2003.02748.x
24. Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–146. doi:10.1097/XEB.0000000000000050
25. Cavanagh M-R, Read J, New B. Sexual abuse inquiry and response: a New Zealand training programme. N Z J Psychol. 2004;33(3):137–144.
26. Du Mont J, Kosa D, Macdonald S, Mason R. The promise of an interactive, online curriculum in improving the competence of those working in healthcare settings to address sexual assault. J Multidiscip Healthc. 2017;10:425–427. doi:10.2147/JMDH.S148075
27. Gore DJ, Prusky M, Solomon CJE, et al. Creation of a medical student training to improve comfort providing trauma-informed care to sexual assault survivors. MedEdPORTAL. 2021;17:11140. doi:10.15766/mep_2374-8265.11140
28. Kennedy KM, Vellinga A, Bonner N, Stewart B, McGrath D. How teaching on the care of the victim of sexual violence alters undergraduate medical students’ awareness of the key issues involved in patient care and their attitudes to such patients. J Forensic Leg Med. 2013;20(6):582–587. doi:10.1016/j.jflm.2013.06.010
29. Siegel M, Gonzalez EC, Wijesekera O, O’Reilly M, March G, Bell S. “On-the-go” training: downloadable modules to educate students in care for sexual assault survivors. Obstetrics Gynecol. 2018;132(Supplement 1):35S–6S. doi:10.1097/01.AOG.0000546598.14219.1a
30. Sullivan R, Clancy T. An experimental evaluation of interdisciplinary training in intervention with sexually abused adolescents. Health Social Work. 1990;15(3):207–214. doi:10.1093/hsw/15.3.207
31. Wen FK, Miller-Cribbs JE, Coon KA, Jelley MJ, Foulks-Rodriguez KA. A simulation and video-based training program to address adverse childhood experiences. Int J Psychiatry Med. 2017;52(3):255–264. doi:10.1177/0091217417730289
32. Barnsley L, Lyon PM, Ralston SJ, et al. Clinical skills in junior medical officers: a comparison of self-reported confidence and observed competence. Med Educ. 2004;38(4):358–367. doi:10.1046/j.1365-2923.2004.01773.x
33. Miller GE. The assessment of clinical skills/competence/performance. Acad Med. 1990;65:s63–s67. doi:10.1097/00001888-199009000-00045
34. Vollmeyer R, Rheinberg F. A surprising effect of feedback on learning. Learn Instruction. 2005;15(6):589–602. doi:10.1016/j.learninstruc.2005.08.001
35. Ball HL. Conducting online surveys. J Hum Lactation. 2019;35(3):413–417. doi:10.1177/0890334419848734
36. Johns R. One size doesn’t fit all: selecting response scales for attitude items. J Election Public Opin Part. 2005;15(2):237–264. doi:10.1080/136898805001788
37. Westland JC, Trujillo CA. Information loss and bias in likert survey responses. PLoS One. 2022;17(7):e0271949. doi:10.1371/journal.pone.0271949
38. Dettori JR. Loss to follow-up. Evid Based Spine Care J. 2011;2(1):7–10.
39. Prestiadi D, Maisyaroh Arifin I, Bhayangkara AN, editors. Meta-analysis of online learning implementation in learning effectiveness.
40. King J, Hill K, Gleason A. All the world’s stage: evaluating psychiatry roleplay based learning for medical students. Australas Psychiatry. 2015;23(1):76–79. doi:10.1177/1039856214563846
41. Nehring WM, Lashley FR. Nursing simulation: a review of the past 40 years. Simul Gaming. 2009;40:528–552. doi:10.1177/1046878109332282
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.