")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Interface Between Motivational Interviewing and Burnout
Authors Hershberger PJ , Flowers SR, Bayless SL, Conway K, Crawford TN
Received 16 November 2023
Accepted for publication 11 February 2024
Published 11 March 2024 Volume 2024:15 Pages 181—187
DOI https://doi.org/10.2147/AMEP.S450179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Paul J Hershberger,1 Stacy R Flowers,1 Sharlo L Bayless,2 Katharine Conway,1 Timothy N Crawford1,3
1Department of Family Medicine, Wright State University Boonshoft School of Medicine, Dayton, OH, USA; 2Wright State University Boonshoft School of Medicine, Dayton, OH, USA; 3Department of Population and Public Health Sciences, Wright State University Boonshoft School of Medicine, Dayton, OH, USA
Correspondence: Paul J Hershberger, Department of Family Medicine, Wright State University Boonshoft School of Medicine, 725 University Blvd, Dayton, OH, 45435, USA, Tel +1 937-245-7223, Fax +1 937-245-7931, Email [email protected]
Background: The contemporary challenges of improving patient engagement in chronic disease management and addressing the growing problem of physician burnout are commonly viewed as separate issues. However, there is extensive evidence that person-centered approaches to patient engagement, such as motivational interviewing (MI), are associated both with better outcomes for patients and improved well-being for clinicians.
Methods: We conducted an exploratory survey study to ascertain whether resident physicians who perceive that they embrace and utilize the MI approach also report less burnout. A total of 318 residents in several specialties were invited via email to complete a 10-question survey about patient engagement and the experience of burnout. Frequencies and percentages were calculated for all categorical/ordinal variables to describe survey participants and question responses. Correlation coefficients were obtained to assess relationships between all burnout and engagement questions.
Results: A total of 79 residents completed the survey (response rate of 24.8%). There was broad agreement about the importance of patient engagement and the use of the MI approach, and approximately 60% of residents indicated that burnout was a problem. Two items related to residents’ perceived use of MI were correlated with feeling a sense of personal accomplishment, one of the protective factors against burnout.
Conclusion: Consistent with other studies indicating that person-centered approaches are associated both with better patient outcomes and provider wellbeing, our data suggest that residents’ self-reported use of the MI approach in patient care may be related to less burnout. It appears that training in the MI approach in graduate medical education may be simultaneously good for patient outcomes and good for resident well-being.
Plain Language Summary: Teaching resident physicians how to take care of their own health, and how to help patients take more responsibility for their health, are typically viewed as two separate challenges. However, studies have shown that patient-centered approaches have benefits both for patient health and clinician health. In our survey of resident physicians, we found that those who say they use motivational interviewing, a patient-centered approach, also report less burnout. This means that teaching resident physicians an effective way to interact with patients is also good for the trainees’ health.
Keywords: patient engagement, physician burnout, motivational interviewing, graduate medical education
Introduction
Two challenges in contemporary medical education are 1) mitigating the development of burnout among resident physicians, and 2) finding adequate time for training in effective patient engagement skills, such as motivational interviewing (MI). The burnout challenge is typically considered a matter of physician wellness, while patient engagement is a clinical care topic, so the two challenges are commonly viewed as separate and require separate commitments of time.
Resident physicians and other practicing physicians are some of the highest-risk groups for burnout and suicide.1–6 There are many contributors to physician burnout, one of which is the lack or loss of meaning in one’s work.7–9 Emphasizing the humanistic aspects of medicine is known to contribute to physician satisfaction and help prevent burnout.8–11
The most central aspect of physician work is the interaction with the patient. There is extensive evidence that humanistic and person-centered approaches are associated with both better health outcomes for patients and improved well-being for providers,12–15 yet such approaches are often perceived as being too time-consuming. Simply educating and advising patients about a treatment plan or lifestyle recommendations is common, and thought to be easier and more efficient for the physician. However, this approach can impede the physician-patient relationship and rarely results in changed behavior, contributing to provider frustration.15,16
MI is a person-centered approach to patient engagement defined as “a collaborative conversation style for strengthening a person’s own motivation and commitment to change”,17 and has been shown to be impactful in eliciting change in a patient’s behavior.18,19 Compared to providers not using MI, those utilizing the approach report less burnout, more treatment team cohesion, and feeling more engaged with patient care.20,21
If utilization of MI is both more effective for patient outcomes and helpful for preventing burnout, it is important to effectively teach and encourage its use in residency programs. Our exploratory study was designed to investigate whether resident physicians who perceive that they embrace and utilize the MI approach also report less burnout.
Methods
Via an email request at a midwestern medical school in the United States, 318 resident physicians representing Emergency Medicine, Family Medicine, Internal Medicine, Obstetrics & Gynecology, Neurology, Pediatrics, and Psychiatry, were invited to complete a 10-question survey developed by the authors that included five questions regarding the use of MI, and five questions related to burnout (eg, emotional exhaustion, cynicism, personal accomplishment).22 The goals in survey development were that it be very brief, include items that reflect commonly measured components of burnout, and include items that would reflect respondent self-perceptions in how they approach discussions of patients’ behavior. Although we did not pilot-test the survey or conduct validity analyses prior to this exploratory study, similar single or few-item burnout questionnaires have been found to be valid.23,24 Because we wanted respondents to remain anonymous, we chose to use self-reported MI behavior rather than actual assessment data obtained from residents who receive MI training in their residency curricula and that not all of the involved residency programs include MI skill development. Survey questions are included in Table 1. Completion of the survey was voluntary, and responses were obtained between February and June of 2021. The study protocol was granted an exemption by the university Institutional Review Board (IRB#06006, June 18, 2019), a determination that was described in the invitation sent to potential participants to complete the survey.
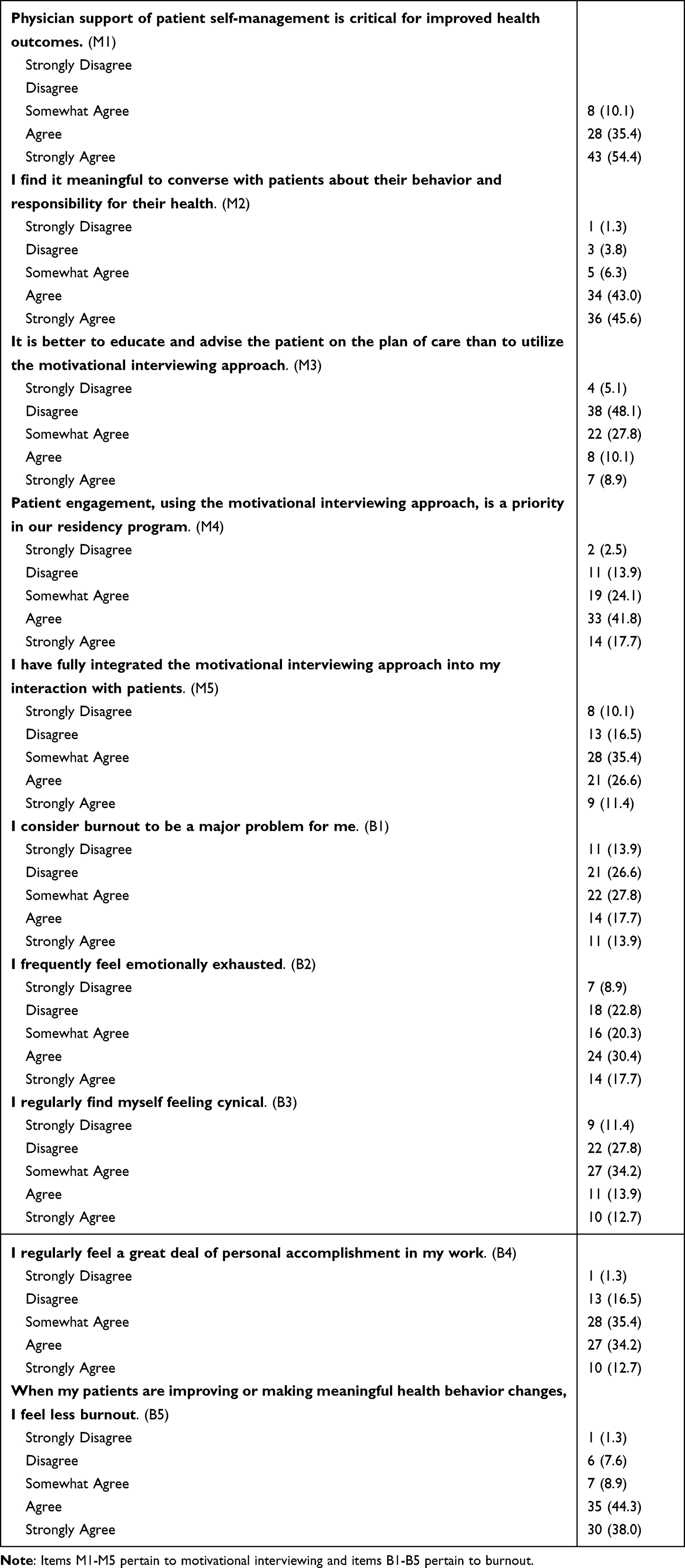 |
Table 1 Descriptive Statistics for Survey Questions (N = 79) |
Data were analyzed using SAS version 9.4 (Cary, NC); frequencies and percentages were calculated for all categorical/ordinal variables to describe the participants and the survey question responses. Spearman correlation coefficients were used to assess the correlation between all individual burnout and MI-related questions. An alpha of <0.05 was used for statistical significance.
Results
Seventy-nine resident physicians across specialties and years of training completed the study survey, a response rate of 24.8%. Characteristics of survey participants are indicated in Table 2. Compared to the demographic characteristics of all residents invited to participate in the study, respondents had slightly higher percentages of females, individualsidentifying as White or Asian, and being in the 30–39 age range. The specialties of Family Medicine and Internal Medicine were also overrepresented among respondents, programs that do include MI skill development in their curricula. Responses to the engagement and burnout questions are included in Table 1. Overall, residents indicated agreement about the importance of patient engagement and the use of the MI approach. Approximately 60% of residents reported that burnout was a problem for them. There was strong agreement that less burnout was experienced when patients make meaningful behavior changes.
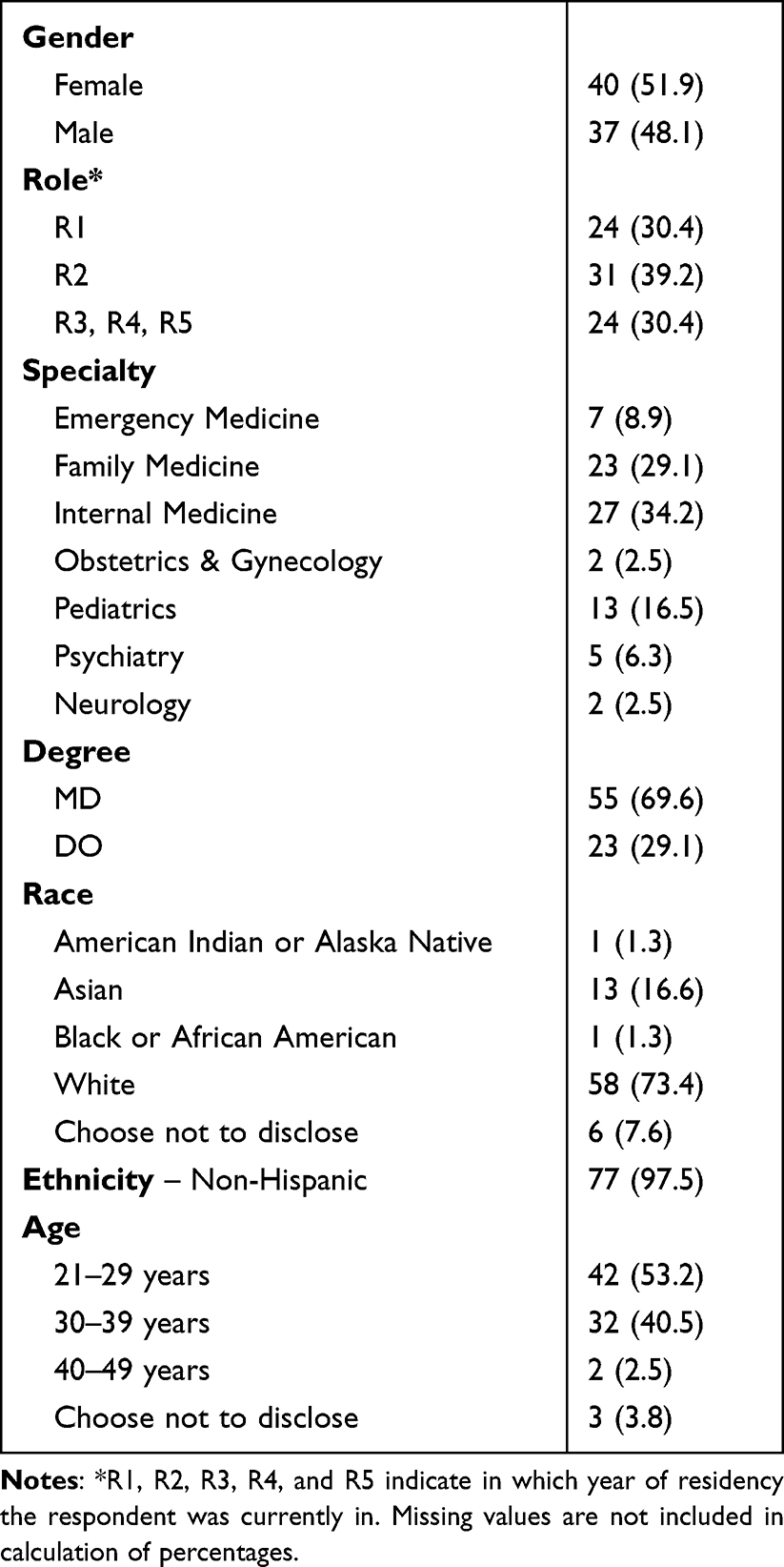 |
Table 2 Descriptive Statistics Among the Participants (N = 79) |
Correlations between the individual burnout and MI questions were calculated and shown in Table 3. Two significant small to moderate, positive correlations were between B4 (“I regularly feel a great deal of personal accomplishment in my work”) and both M4 (rs = 0.257, p < 0.05) and M5 (rs = 0.306, p < 0.01) (“Patient engagement, using the motivational interviewing approach, is a priority in our residency program” and “I have fully integrated the motivational interviewing approach into my interaction with patients”, respectively).
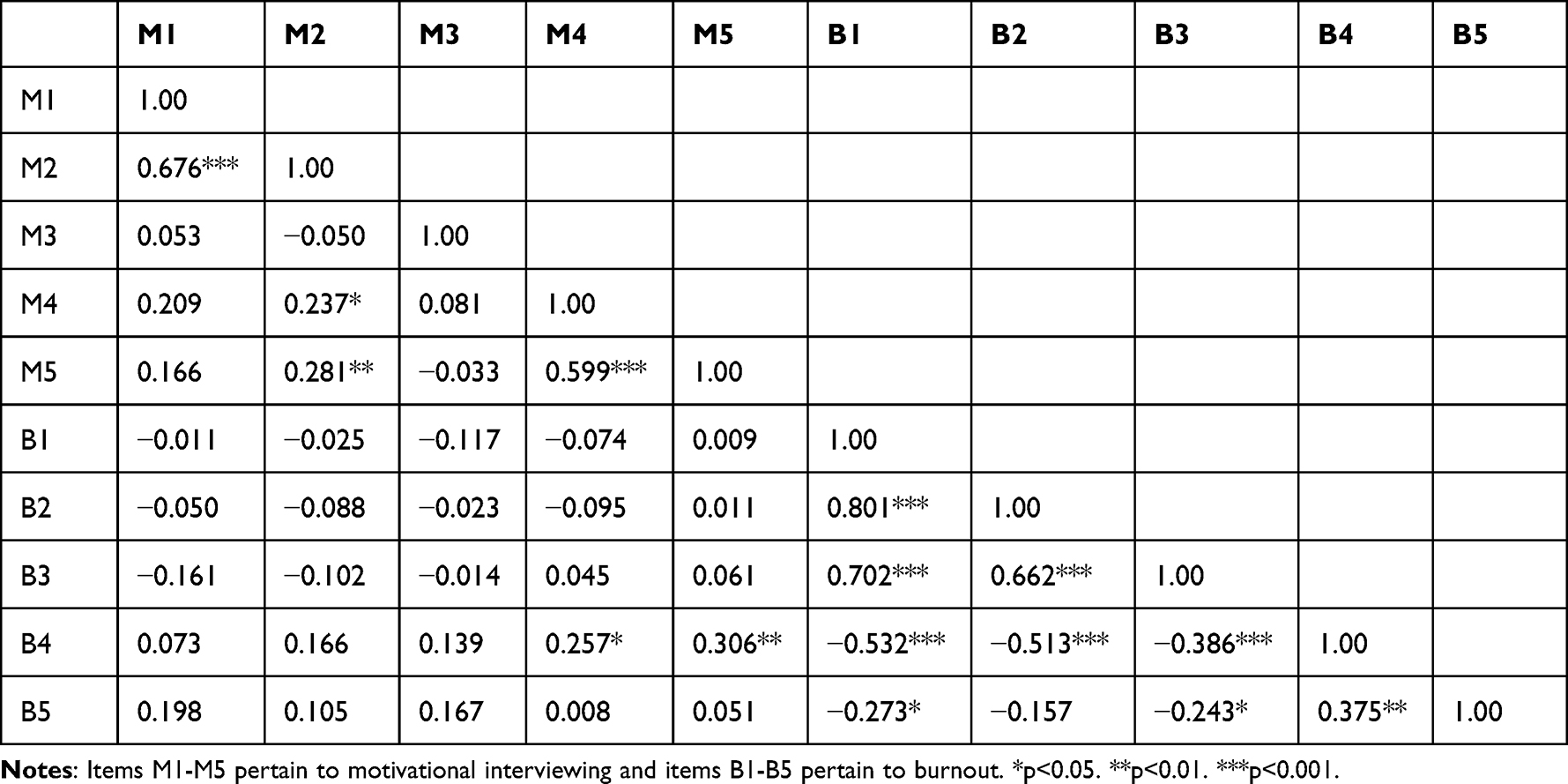 |
Table 3 Spearman Correlations Among All Items |
A secondary analysis was conducted to determine whether there were differences in survey results from residents in programs that do or do not explicitly include MI training in their curricula. The only question where results were statistically different was item B5 (“When my patients are improving or making meaningful health behavior changes, I feel less burnout”); those from programs that teach MI were more likely to strongly agree with the statement.
Discussion
There are significant correlations in our exploratory study which suggest that resident physicians who embrace patient engagement through the MI approach, and whose residency programs promote the use of the MI approach, feel more accomplishment in their clinical work. The notion that prioritizing and integrating MI is associated with feeling personal accomplishment in one’s work is consistent with studies indicating that providers who use MI tend to be more satisfied and have better patient interaction.15,20,21 Our results, therefore, may suggest that utilization of the MI approach can have protective benefits against physician burnout and that these benefits can be appreciated in graduate medical education. Residency programs that promote patient engagement with the use of the MI approach may be increasing the likelihood that residents will actually observe meaningful health behavior change by patients, whereas programs where the culture is to simply tell patients what to do (ie, educate and advise) may be less likely to see such progress with patients. Furthermore, as the secondary analysis suggests, those residents seeing patients’ progress may recognize this as helping mitigate their own burnout, possibly because the collaborative resident-patient relationships promoted with the MI approach are meaningful and satisfying.
Our study did not include objective assessment of the actual implementation of the MI approach by residents, so it is important to note the self-report nature of our data with the possibility for social desirability bias. Indeed, residents more strongly endorsed the importance of patient engagement and MI than was expected based on the observations of those of us who work with residents, so our results may exaggerate the actual extent to which the MI approach is practiced. Nearly 80% of participating residents were from Internal Medicine, Family Medicine, and Pediatrics, programs that include a required MI module in their curricula, which may present some self-selection bias on the part of those who chose to participate. Responses to survey questions regarding burnout were similar to other burnout data routinely obtained in the Family Medicine Residency program.
Additional limitations of our exploratory study include a small sample size, the use of a brief non-validated survey developed by the authors, and a low response rate. Some degree of bias was likely with self-reported results, particularly with respect to the use of the MI approach. Subsequent studies should make use of more objective indicators of MI skills and utilization, and obtain a larger sample of residents.
There is evidence that MI can be effectively taught to residents,25 although it does require time and repeated practice, and promoting it as a long-term approach in patient interactions remains a challenge.26 Another ongoing challenge is to implement strategies that can mitigate burnout. At first glance these may seem to be separate endeavors, but the results of our exploratory study suggest that training residents to use the MI approach may itself be a skill that can help mitigate burnout.
Conclusion
One of the challenges in graduate medical education is finding the time to train residents in effective patient engagement, while another challenge is to implement strategies that can mitigate burnout. Although at first glance these may seem to be separate endeavors, the results of our pilot study suggest that training residents to use the MI approach may itself be a skill that can help mitigate burnout. This potential interface between what is good for patient care and outcomes, and what is good for the well-being of the physician workforce deserves further consideration and exploration.
Abbreviation
MI, Motivational Interviewing.
Ethics Approval
The study protocol was granted an exemption by the Wright State University Institutional Review Board (IRB#06006, June 18, 2019). The invitation to participate in the survey study included this information and completion of the survey was how participants provided informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed to submit to the current journal; and agree to be accountable for all aspects of the work.
Funding
There is no funding source associated with the content or preparation of this manuscript.
Disclosure
The authors do not have any conflicts of interest to disclose for this work.
References
1. Kane L. ‘Death by 1000 Cuts’: Medscape national physician burnout & suicide report 2021; 2021. Available from: https://www.medscape.com/slideshow/2021-lifestyle-burnout-6013456#2.
2. Murphy B How often do physicians and medical students die of suicide? American Medical Association; 2019. Available from: https://www.ama-assn.org/practice-management/physician-health/how-often-do-physicians-and-medical-students-die-suicide.
3. Dutheil F, Aubert C, Pereira B, et al. Suicide among physicians and health-care workers: a systematic review and meta-analysis. PLoS One. 2019;14(12):e0226361. doi:10.1371/journal.pone.0226361
4. Card AJ. Physician burnout: resilience training is only part of the solution. Ann Fam Med. 2018;16(3):267–270. doi:10.1370/afm.2223
5. Kung A, Cheung T, Knox M, et al. Capacity to address social needs affects primary care clinician burnout. Ann Fam Med. 2019;17(6):487–494. doi:10.1370/afm.2470
6. Nedrow A, Steckler N, Hardman J. Physician resilience and burnout: can you make the switch? Fam Pract Manag. 2013;20(1):25–30.
7. Dobler CC, West CP, Montori VM. Can shared decision making improve physician well-being and reduce burnout? Cureus. 2017. doi:10.7759/cureus.1615
8. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J of Intern Med. 2018;283(6):516–529. doi:10.1111/joim.12752
9. Gregory ST, Menser T. Burnout among primary care physicians: a test of the areas of worklife model. J Healthc Manag. 2015;60(2):133–148. doi:10.1097/00115514-201503000-00009
10. Serwint JR, Stewart MT. Cultivating the joy of medicine: a focus on intrinsic factors and the meaning of our work. Curr Probl Pediatr Adolesc Health Care. 2019;49(12):100665. doi:10.1016/j.cppeds.2019.100665
11. Hooker SA, Post RE, Sherman MD. Awareness of meaning in life is protective against burnout among family physicians: a CERA study. Fam Med. 2020;52(1):11–16. doi:10.22454/FamMed.2019.562297
12. Barnett KAG. In pursuit of the fourth aim in health care: the joy of practice. Med Clin North Am. 2017;101(5):1031–1040. PMID: 28802466. doi:10.1016/j.mcna.2017.04.014
13. Lown BA, Shin A, Jones RN. Can organizational leaders sustain compassionate, patient-centered care and mitigate burnout? J Healthc Manag. 2019;64(6):398–412. doi:10.1097/JHM-D-18-00023
14. Flowers SR, Hershberger PJ. Commentary: individual and organizational strategies for physician well-being. Curr Probl Pediatr Adolesc Health Care. 2019;49(12):100687. PMID: 31708367. doi:10.1016/j.cppeds.2019.100687
15. Hershberger PJ, Bricker DA, Conway K, Torcasio MH. Turning “lose-lose” into “win-win”: what is good for them is good for us! Med Sci Educ. 2021;31:1177–1181. doi:10.1007/s40670-021-01280-4
16. Levy AG, Scherer AM, Zikmund-Fisher BJ, Larkin K, Barnes GD, Fagerlin A. Prevalence of and factors associated with patient nondisclosure of medically relevant information to clinicians. JAMA Netw. 2018;1(7):e185293. doi:10.1001/jamanetworkopen.2018.5293
17. Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. New York: Guilford; 2013.
18. Szczekala K, Wiktor K, Kanadys K, et al. Benefits of motivational interviewing application for patients and healthcare professionals. Pol J Public Health. 2018;128(4):170–173. doi:10.2478/pjph-2018-0034
19. VanBuskirk KA, Wetherell JL. Motivational interviewing with primary care populations: a systematic review and meta-analysis. J of Behav Med. 2014;37(4):768–780. doi:10.1007/s10865-013-9527-4
20. Pollak KI, Nagy P, Bigger J, et al. Effect of teaching motivational interviewing via communication coaching on clinician and patient satisfaction in primary care and pediatric obesity-focused offices. Patient Educ Couns. 2016;99(2):300–303. doi:10.1016/j.pec.2015.08.013
21. Endrejat PC, Kauffeld S. Learning motivational interviewing: prospects to preserve practitioners’ well-being. Int J Workplace Health Manag. 2020;14(1):1–11. doi:10.1108/IJWHM-03-2020-0041
22. Drybye LN, Hunderfund ANL, Winters RC, et al. The relationship between burnout and help-seeking behaviors, concerns, and attitudes of residents. Acad Med. 2021;96(5):701–708. doi:10.1097/ACM.0000000000003790
23. Rohland BM, Druse GR, Rohrer JE. Validation of a single-item measure of burnout against the Maslach Burnout inventory among physicians. Stress Health. 2004;20(2):75–79. doi:10.1002/smi.1002
24. West CP, Dyrbye LN, Sloan JA, Shanafelt TD. Single item measures of emotional exhaustion and depersonalization are useful for assessing burnout in medical professionals. J Gen Intern Med. 2009;24(12):1318–1321. doi:10.1007/s11606-009-1129-z
25. Dunhill D, Schmidt S, Klein R. Motivational interviewing interventions in graduate medical education: a systematic review of the evidence. J Grad Med Educ. 2014;2:222–236. doi:10.4300/JGME-D-13-00124.1
26. Hall K, Staiger PK, Simpson A, Best D, Lubman DI. After 30 years of dissemination, have we achieved sustained practice change in motivational interviewing? Addiction. 2015;111:1144–1150. doi:10.1111/add.13014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.