")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Relationship Between Cognitive Load Theory, Intrinsic Motivation and Emotions in Healthcare Professions Education: A Perspective on the Missing Link
Authors Patel D , Alismail A
Received 27 September 2023
Accepted for publication 8 January 2024
Published 19 January 2024 Volume 2024:15 Pages 57—62
DOI https://doi.org/10.2147/AMEP.S441405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Dhruvita Patel,1 Abdullah Alismail1,2
1Department of Cardiopulmonary Sciences, School of Allied Health Professions, Loma Linda University Health, Loma Linda, CA, USA; 2Department of Medicine, School of Medicine, Loma Linda University Health, Loma Linda, CA, USA
Correspondence: Abdullah Alismail, Cardiopulmonary Sciences and Medicine, Loma Linda University, Email [email protected]
Abstract: Cognitive Load Theory (CLT) is one of the key cognitive theories that have been used to assess learners’ information and working memory load. CLT has been applied to Simulation Based Education (SBE) and optimizing instructional design. However, a challenge that occurs is that these high-fidelity simulations and mannequins of critically ill patients can elicit negative emotions in learners which can unfavorably impact the learning process. There is also a potential for cognitive overload if the simulation is more authentic and requires more dynamic interactions and lead to high levels of anxiety due to a novel learning environment, which can also have detrimental effects on learning process. Hence, it is critical for health professional educators (HPE) to know how to minimize cognitive load to improve learning as a professional in a workplace setting. The literature on the role of emotions, intrinsic motivation, cognitive load is scarce in HPE literature. Specifically when not being studied together at once since they move dynamically together and affect the learning for the learner. Therefore, the purpose of this perspective paper is to cover the gap in the literature and propose a framework and recommendation for future HPE research.
Keywords: motivation, simulation-based education, cognitive load, emotions, situational motivation
Overview and Introduction
Education science can be broadly described as the study of improving teaching process. It includes research of different teaching methods and how to improve them for effective learner outcomes.1,2 Therefore, studies that evaluate and study neuro and behavior aspects of learning such as cognition, emotions, and motivation are showing interesting evidence of how learners think and learn, especially in medical education clinical settings.3–8 The aim of the perspective paper is to review and highlight existing research on Cognitive Load Theory (CLT), emotions, and intrinsic motivation among health care learners in a simulation-based environment. As well as identify limitation and propose a recommendation to the future medical education scholars to consider based on the identified limitation.
Cognitive Load
CLT was developed by John Sweller in 1988, who described “cognitive load” as the amount of information working memory can hold at one time. Sweller suggested that since working memory has limited capacity, instructional methods need to be effective, and they should not overload the memory with unnecessary activities and information that do not contribute to learning.9,10 CLT builds on a widely accepted model of human information processing in the brain which has three main parts: sensory memory, working memory and long-term memory. Sensory memory filters out unnecessary sensory information that we are constantly bombarded with but keeps important items long enough to pass to working memory.11,12 Working memory can hold 7 ± 2 items or information at a time.13 As the brain processes this information, it categorizes it into “schemas” or knowledge structures, as it becomes stored in the long-term memory.11 CLT suggests that because working memory is limited, instructional techniques and learning experiences should be designed to reduce the working memory “load” and make schema formation efficient. In other words, since the brain can only hold so much information at once, instructors need to be intentional with what they teach students and what they ask them to do. There are three types of cognitive load: 1) Intrinsic, Extraneous, and Germane loads. Intrinsic cognitive load (ICL) is directly relevant to learning and the content. Extraneous cognitive load (ECL) refers to the source of demand on working memory that is unnecessary for learning. Germane load (GL) refers to the mental resource that facilitates schemas to store in long-term memory.14–16 A common validated instrument that is used to measure cognitive load is a subjective self-report 10-item instrument developed by Leppink et al17–20 The multidimensional scale assesses ICL based on complexity of the instructional content, ECL based on participants’ perceptions of the negative attributes of information presented during instruction, and GL based on perceived contributions of the instructions and explanations during the learning activities. Responses are recorded on a 9-point scale where 0 = very very low mental effort and 9 = very very high mental effort.21 Studies reported that measuring the cognitive loads after an instructional process can provide useful information about learners, and the issue of variability in learning outcomes that exists between different learners despite receiving similar instruction.20
Introduction to the Problem: Simulation Based Education Based on Cognitive Load Theory
Simulation Based Education (SBE) has been known to be an effective and preferred instructional technique in health professions. A systematic review revealed that simulation positively has large effects on learner’s knowledge, skills, and patient outcomes.22 CLT has been applied to SBE to optimize instructional design for improved learning outcomes.23–25 Clinical skills acquisition is a common learning objective for medical education laboratory skills and simulation.26,27 In the simulation world, the modern mannequins are a sophisticated way to create real time changes in hemodynamics, vital signs and respond to clinical interventions. It creates a safe place for interventions to be performed and practice by students that are deemed dangerous to practice on actual patients and creates a safe learning environment.23 However, there is a potential for cognitive overload if the simulation is more authentic and requires more dynamic interactions, which can impair learning.28 A study by Fraser et al demonstrated that high ECL during training with clinical simulation is associated with decreased learning and impaired performance of clinical skills.29 One of the ways ECL can be reduced is by introducing learners to the simulation environment in advance, since being in an unfamiliar environment can consume more cognitive resources, as learners may not know what resources are available in the room.30 Hence, it is significant to tailor ICL to the level of the learner, minimize ECL, and optimize GL to enhance learning during simulation. However, more areas should be considered that have not been explored simultaneously with CL enough in the literature, such as motivation and emotions, that ultimately affect learning outcomes. This is mostly due to the dynamic effect nature of these factors on learning.
Cognitive Load Theory and Motivation
Motivation has been dichotomized for several decades into intrinsic and extrinsic categories.31 Intrinsic motivation comes from carrying out a task solely for enjoyment and out of personal interest. Extrinsic motivation, on the other hand, pertains to behaviors where goal of action extends beyond the task or activity itself. Another terminology coined is situational motivation, which refers to the motivation that comes when engaging in an activity and is the “here and now” of motivation.31
It is important to assess a person’s situational (or intrinsic) motivation to understand their current self-regulatory process. A validated self-report scale called the Situational Motivation Scale (SIMS) has been used to assess participant’s reaction towards an activity at any given time. The scores range from 1 (corresponds not at all) to 7 (corresponds exactly to a given situation.32 A study by Escher et al utilized SIMS to assess medical students self-reported motivation to participate in simulation-based teamwork, and found that students’ patient safety attitudes toward patient safety had positive correlation to motivation.33 Another prospective cohort study that utilized SIMS found that a repetitive SBE had no significant effect on situational motivation, but after three-day bedside teaching, the external and identified motivation of 3rd year medical students decreased. The authors Moll-Khosrawi et al shown the light on the importance of preventing the unintended decrease of intrinsic motivation in medical students, and that they should be supervised and tactically introduced to bedside teaching.34 Additionally, a recent study by Hadie et al revealed CLT-based online lectures promoted the students’ comprehension of the lecture content, self-perceived learning, engagement toward the learning material, and motivation to learn.35 The study also revealed that the students’ intrinsic and extraneous cognitive loads had decreased post CLT-based lecture and promoted learning motivation.35 The previously noted studies revealed interesting and significant findings about motivation and learning. However, to the author’s knowledge, the effects of motivational dimension of learning in relation to SBE and CLT in medical education have not been explored in detail and needs further investigations.
Cognitive Load Theory and Emotion
Emotions have significant influence on learning, and critics suggest that emotion and cognition are integrated in the brain that it is not possible to separate the emotion and learning since “complex cognitive-emotional behavior emerges from the rich, dynamic interactions between brain networks.”29 Plass et al categorize emotions as a source of extraneous cognitive load.36 They argue negative emotions can lead to allocation of resources ie, task irrelevant processing of information, that is not directly related to learning outcome.37 Task extra processing refers to processes done for emotion regulation that use up cognitive resources, and since they are not contributing to the learning goal, they are categorized as extraneous cognitive load.29 Clinical simulations contain elements that can trigger anxiety and other negative emotions due to overload of clinical data, associated assessments and overall instructions provided, which consume the working memory capacity.37–41 A well-known validated psychometric self-report scale used to assess emotions is the Positive and Negative Affect Schedule (PANAS).42 Several studies have explored this tool in various healthcare professions.26,43–47 For example, a study that utilized PANAS and virtual reality (VR) as a teaching tool revealed that VR significantly modified learners’ emotions and reinforced positive emotional states. VR facilitated the teaching-learning process and made it possible for learners to practice skills in simulated and safer conditions and made the didactic process more attractive, thereby influencing learners’ emotions positively.48 However, high-fidelity simulations of life-or-death scenarios can influence emotional state and impact ECL. A randomized control trial demonstrated that exposing students to unexpected death of a simulated patient increased total CL and they had poorer learning outcomes.49 Another study tested the effects of emotional competence (EC) level on simulated emergency care situations in medical residents. They found that subjects with high EC level were better able to manage negative affect, and able to put their medical knowledge to work and explore alternative diagnoses.45 Hence, a concern during high-fidelity simulations and mannequins of critically ill patients could elicit negative emotions in learners which can unfavorably impact the learning process.
To place all of the presented variables together, in Figure 1 we shows how these variables work together to affect learners while being in a clinical environment in terms of interaction and relationship [direct or inverse]. They work dynamically together as well as affect each other and eventually impact learning [positively and/or negatively].
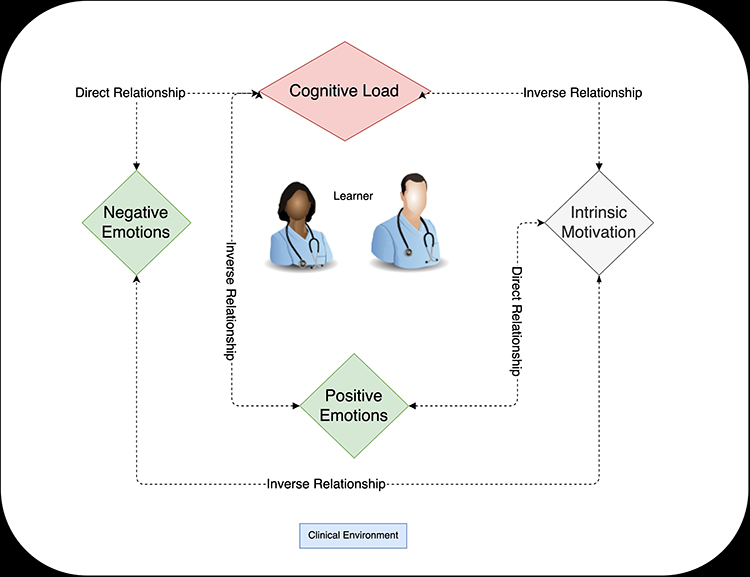 |
Figure 1 This figure shows how all key variables are linked and interact with each other around the learner in terms of relationship (direct or inverse). |
Limitations:
As previously mentioned, limitations in existing studies can be summarized and combined where the link between intrinsic motivation and emotions have not yet been explored in regards with CLT in healthcare profession students. This limitation can be mitigated by shifting the focus on how to provide effective SBE and clarifying features that optimize learning outcomes using the these variables together effectively.
Conclusion and Recommendation
The aim of this perspective article was to highlight the limitations and challenges that arise during SBE of health profession students in relation to CLT, emotions and motivation. Motivation has been shown to impact learning outcomes in SBE.34 As well, emotions can act as ECL in high fidelity simulations and lead to poor learning outcomes.50 The specific area of CLT in relation to intrinsic motivation and emotions is worth exploring further in the literature among selected professions such as respiratory therapist and nursing as research is showing that promoting motivation and a growth mindset can reduce cognitive load. These two professions work in a high intense complex environment (ie intensive care unit and emergency rooms) where these factors are major role players for learning. In addition, since increased negative emotions associated with simulation can increase ECL and lead to poorer learning outcomes, it is crucial for clinical educators to work on ways to minimize ECL. Since healthcare professionals work in high-stress situations and stimulating environments, there cognitive load is likely to be constantly on the high end. Therefore, it is noteworthy to minimize cognitive load to improve learning as a professional in a workplace setting. This can be achieved by investigating the link between CTL, motivation, and emotions, specifically in a simulation-based environment and followed in real setting longitudinally.
Disclosure
All authors report no conflict of interest.
References
1. Immordino-Yang MH, We Feel DA. Therefore we learn: the relevance of affective and social neuroscience to education. Mind Brain Educ. 2007;1(1):3–10.
2. Tohidi H, Jabbari MM. The effects of motivation in education. Procedia Soc Behav Sci. 2012;31:820–824. doi:10.1016/j.sbspro.2011.12.148
3. Ajjawi R, Olson RE, McNaughton N. Emotion as reflexive practice: a new discourse for feedback practice and research. Med Educ. 2022;56(5):480–488. doi:10.1111/medu.14700
4. Duffy MC, Lajoie SP, Pekrun R, Lachapelle K. Emotions in medical education: examining the validity of the Medical Emotion Scale (MES) across authentic medical learning environments. Learn Instr. 2020;70:101150. doi:10.1016/j.learninstruc.2018.07.001
5. Dworkis DA, Jain A, Wolfe M, Sanko S, Arora S. Cognitive load during training for out‐of‐department emergency responses. AEM Educ Train. 2022;6(3):e10742. doi:10.1002/aet2.10742
6. Greer SK, Jeffe DB, Manga A, Murray DJ, Emke AR. Cognitive load assessment scales in simulation: validity evidence for a novel measure of cognitive load types. Simul Healthc J Soc Simul Healthc. 2023;18(3):172–180. doi:10.1097/SIH.0000000000000665
7. Huckaby LV, Cyr AR, Handzel RM, et al. Postprocedural cognitive load measurement with immediate feedback to guide curriculum development. Ann Thorac Surg. 2022;113(4):1370–1377. doi:10.1016/j.athoracsur.2021.05.086
8. Mills LM, Boscardin C, Joyce EA, ten Cate O, O’Sullivan PS. Emotion in remediation: a scoping review of the medical education literature. Med Educ. 2021;55(12):1350–1362. doi:10.1111/medu.14605
9. Sashitzky I. The Science of Education; 2019.
10. What is Education Sciences ?; 2022. Available from: https://advise.education.uci.edu/what-is-education-sciences.html.
11. Cognitive Load Theory (John Sweller); 2022. Available from: https://www.instructionaldesign.org/theories/cognitive-load/.
12. Sweller J CHAPTER TWO - Cognitive Load Theory. In: Psychology of learning and motivation. Academic Press; 2011:37–76. Available from: https://www.sciencedirect.com/science/article/pii/B9780123876911000028.
13. Miller GA. The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychol Rev. 1956;63(2):81–97. doi:10.1037/h0043158
14. Kirschner PA. Cognitive load theory: implications of cognitive load theory on the design of learning. Learn Instr. 2002;12(1):1–10. doi:10.1016/S0959-4752(01)00014-7
15. Van Merriã«nboer JJG, Sweller J. Cognitive load theory in health professional education: design principles and strategies: cognitive load theory. Med Educ. 2010;44(1):85–93. doi:10.1111/j.1365-2923.2009.03498.x
16. Cognitive Load Theory; 2022. Available from: https://www.mindtools.com/aqxwcpa/cognitive-load-theory.
17. Hadie SNH, Yusoff MSB. Assessing the validity of the cognitive load scale in a problem-based learning setting. J Taibah Univ Med Sci. 2016;11(3):194–202.
18. Leppink J, Paas F, van GT, van der VCPM, van MJJG. Effects of pairs of problems and examples on task performance and different types of cognitive load. Learn Instr. 2014;30:32–42. doi:10.1016/j.learninstruc.2013.12.001
19. Bergman EM, de Bruin ABH, Vorstenbosch MATM, et al. Effects of learning content in context on knowledge acquisition and recall: a pretest-posttest control group design. BMC Med Educ. 2015;15(1):133. doi:10.1186/s12909-015-0416-0
20. Klepsch M, Schmitz F, Seufert T. Development and validation of two instruments measuring intrinsic, extraneous, and germane cognitive load. Front Psychol. 2017;8:1997. doi:10.3389/fpsyg.2017.01997
21. Andersen MS, Makransky G. The validation and further development of a multidimensional cognitive load scale for virtual environments. J Comput Assist Learn. 2021;37(1):183–196. doi:10.1111/jcal.12478
22. Cook DA, Hamstra SJ, Brydges R, et al. Comparative effectiveness of instructional design features in simulation-based education: systematic review and meta-analysis. Med Teach. 2013;35(1):e867–98. doi:10.3109/0142159X.2012.714886
23. Fraser KL, Ayres P, Sweller J. Cognitive load theory for the design of medical simulations. Simul Healthc J Soc Simul Healthc. 2015;10(5):295–307.
24. Meguerdichian M, Walker K, Bajaj K. Working memory is limited: improving knowledge transfer by optimising simulation through cognitive load theory. BMJ Simul Technol Enhanc Learn. 2016;2(4):131–138. doi:10.1136/bmjstel-2015-000098
25. Adams T. The application of cognitive load theory to dual-task simulation training. Simul Healthc J Soc Simul Healthc. 2016;11(1):66–67. doi:10.1097/SIH.0000000000000143
26. Lumowa K, Lui KL, Daher N, Baek C, Tan LD, Alismail A. Evaluation of tracheostomy suctioning procedure among nursing and respiratory therapy students: wearable manikin vs. standard manikin. Front Med. 2023;2023:10.
27. Rossettini G, Rondoni A, Palese A, et al. Effective teaching of manual skills to physiotherapy students: a randomised clinical trial. Med Educ. 2017;51(8):826–838. doi:10.1111/medu.13347
28. Brown JS, Collins A, Duguid P. Situated cognition and the culture of learning. Educ Res. 1989;18(1):32–42. doi:10.2307/1176008
29. Fraser K, Ma I, Teteris E, Baxter H, Wright B, McLaughlin K. Emotion, cognitive load and learning outcomes during simulation training: emotion and cognitive load during simulation. Med Educ. 2012;46(11):1055–1062. doi:10.1111/j.1365-2923.2012.04355.x
30. Rudolph JW, Raemer DB, Simon R. Establishing a safe container for learning in simulation: the role of the presimulation briefing. Simul Healthc J Soc Simul Healthc. 2014;9(6):339–349. doi:10.1097/SIH.0000000000000047
31. Feldon DF, Callan G, Juth S, Jeong S. Cognitive load as motivational cost. Educ Psychol Rev. 2019;31(2):319–337. doi:10.1007/s10648-019-09464-6
32. Guay F, Vallerand RJ, Blanchard C. No title found. Motiv Emot. 2000;24(3):175–213. doi:10.1023/A:1005614228250
33. Escher C, Creutzfeldt J, Meurling L, Hedman L, Kjellin A, Felländer-Tsai L. Medical students’ situational motivation to participate in simulation based team training is predicted by attitudes to patient safety. BMC Med Educ. 2017;17(1):37. doi:10.1186/s12909-017-0876-5
34. Moll-Khosrawi P, Cronje JS, Zöllner C, Kubitz JC, Schulte-Uentrop L. Understanding how the motivational dimension of learning is influenced by clinical teaching in medical education: a prospective cohort study. Ann Med Surg. 2021;2021:65.
35. Hadie SNH, Tan VPS, Omar N, Nik Mohd Alwi NA, Lim HL, Ku Marsilla KI. COVID-19 disruptions in health professional education: use of cognitive load theory on students’ comprehension, cognitive load, engagement, and motivation. Front Med. 2021;8:739238. doi:10.3389/fmed.2021.739238
36. Plass JL, Kalyuga S. Four ways of considering emotion in cognitive load theory. Educ Psychol Rev. 2019;31(2):339–359. doi:10.1007/s10648-019-09473-5
37. Edwards MS, Moore P, Champion JC, Edwards EJ. Effects of trait anxiety and situational stress on attentional shifting are buffered by working memory capacity. Anxiety Stress Coping. 2015;28(1):1–16. doi:10.1080/10615806.2014.911846
38. Keitel A, Ringleb M, Schwartges I, et al. Endocrine and psychological stress responses in a simulated emergency situation. Psychoneuroendocrinology. 2011;36(1):98–108. doi:10.1016/j.psyneuen.2010.06.011
39. Harvey A, Nathens AB, Bandiera G, LeBlanc VR. Threat and challenge: cognitive appraisal and stress responses in simulated trauma resuscitations: appraisal and stress in simulated trauma resuscitations. Med Educ. 2010;44(6):587–594. doi:10.1111/j.1365-2923.2010.03634.x
40. Lyndon MP, Strom JM, Hussain M, et al. The relationship between academic assessment and psychological distress among medical students: a systematic review. Perspect Med Educ. 2014;3(6):405–418. doi:10.1007/S40037-014-0148-6
41. Stein C. The effect of clinical simulation assessment on stress and anxiety measures in emergency care students. Afr J Emerg Med. 2020;10(1):35–39. doi:10.1016/j.afjem.2019.12.001
42. Crawford JR, Henry JD. The positive and negative affect schedule (PANAS): construct validity, measurement properties and normative data in a large non-clinical sample. Br J Clin Psychol. 2004;43(3):245–265. doi:10.1348/0144665031752934
43. Toohey S, Wray A, Hunter J, et al. Comparing the psychological effects of manikin-based and augmented reality–based simulation training: within-subjects crossover study. JMIR Med Educ. 2022;8(3):e36447. doi:10.2196/36447
44. Rama A, Neiman N, Burdsall K, et al. Virtual immersion into a poorly-managed medical crisis worsens subsequent performance: a randomized, controlled trial. Clin Simul Nurs. 2022;70:47–55. doi:10.1016/j.ecns.2022.06.008
45. Bourgeon L, Bensalah M, Vacher A, Ardouin JC, Debien B. Role of emotional competence in residents’ simulated emergency care performance: a mixed-methods study. BMJ Qual Saf. 2016;25(5):364–371. doi:10.1136/bmjqs-2015-004032
46. Volonte M, Babu SV, Chaturvedi H, et al. Effects of virtual human appearance fidelity on emotion contagion in affective inter-personal simulations. IEEE Trans Vis Comput Graph. 2016;22(4):1326–1335. doi:10.1109/TVCG.2016.2518158
47. Rogers T, Andler C, O’Brien B, van Schaik S. Self-reported emotions in simulation-based learning: active participants vs. Observers Simul Healthc J Soc Simul Healthc. 2019;14(3):140–145.
48. Ślósarz L, Jurczyk-Romanowska E, Rosińczuk J, Kazimierska-Zając M. Virtual reality as a teaching resource which reinforces emotions in the teaching process. SAGE Open. 2022;12(3):215824402211180. doi:10.1177/21582440221118083
49. Fraser K, Huffman J, Ma I, et al. The emotional and cognitive impact of unexpected simulated patient death: a randomized controlled trial. Chest. 2014;145(5):958–963. doi:10.1378/chest.13-0987
50. Fredericks S, ElSayed M, Hammad M, et al. Anxiety is associated with extraneous cognitive load during teaching using high-fidelity clinical simulation. Med Educ Online. 2021;26(1):1994691. doi:10.1080/10872981.2021.1994691
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.