")
Back to Journals » Advances in Medical Education and Practice » Volume 15
What Matters Most: Determinants Associated with the Selection of Medical Residencies in Qatar
Authors Kane T , Ford J , Al Saady RM , Vranic S , Musa OAH, Suliman S
Received 8 September 2023
Accepted for publication 20 December 2023
Published 28 February 2024 Volume 2024:15 Pages 141—151
DOI https://doi.org/10.2147/AMEP.S429758
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Tanya Kane,1 Jason Ford,2 Rafif Mahmood Al Saady,1 Semir Vranic,1 Omran AH Musa,3 Shireen Suliman4,5
1College of Medicine, QU Health, Qatar University, Doha, Qatar; 2Department of Pathology, Sidra Medicine, Doha, Qatar; 3Department of Disease Control, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, UK; 4Medicine Department, Hamad Medical Corporation, Doha, Qatar; 5School of Health Professions Education, Maastricht University, Maastricht, the Netherlands
Correspondence: Shireen Suliman, Email [email protected]
Purpose: There have been several studies into medical student career decision making in occidental countries (eg US, UK), but medical career selection in a Middle Eastern context has not been as well studied. This study aims to explore determinants underpinning medical students’ residency choice in Qatar.
Patients and methods: During the Fall semester of the 2022– 2023 academic year, all (n=358) medical students from the College of Medicine at Qatar University were invited to participate in an online explorative questionnaire about students’ career choices and the factors determining their selection.
Results: Of the 358 students, 184 responded (51%). Respondents had a mean age of 20 years; the majority were female (73.9%), Qatari (54.3%), unmarried (97.3%), and enrolled in a pre-clerkship year (55.0%). The most important career determinant was specialty-specific factors. The relative importance of other determinants differed by gender and stage of training. Among our respondents, male students were more likely to rate role models and influencers as being important to their choice, while female students and Qatari students overall were more likely to cite societal obligation. Medical students in Qatar seemed to have career preferences in mind upon entry into medical education. Later-year students were more likely to identify the importance of work-life balance and place of practice, but were less likely to rank prestige and income as an important determinant.
Conclusion: The results of this baseline study suggest that socioeconomic and cultural context influence medical student career decisions.
Keywords: career choice, specialty selection, medical students, medical education, residency, Qatar
Introduction
The choice of medical specialty is a complex decision that has considerable influence on the trajectory of students’ lives and careers as well as the nation’s medical workforce. Earlier studies suggest many medical students enter medical school with a specialty in mind.1–3 Factors influencing residency career choices are complex and vary across various contexts.4 While gender has been found to play a decisive factor,4–6 a regional study identified individual characteristics and specialty-related lifestyles as important selection drivers but pointed to the need for further research to examine female preferences in the region.6,7
Schmidt et al’s systematic review underscores the role of mentorship, stereotypes, clinical experience, the timing of exposure, and personal factors in US students’ decisions to undertake surgical residencies.8 In addition, lifestyle and work-life balance, societal orientation, prestige and income, place of practice, scope of practice, role models, university influence, and interest in the discipline are key considerations.4
The intellectual content of the preferred specialty is also cited as an important consideration among students.5,9,10 In Kuwait, students ranked positive treatment outcomes as a major determinant in students’ career choices.11 The quality of the residency program itself was another influential factor identified in a recent study.12 With both contextual and temporal variables at play, no consensus has been reached regarding a definitive set of influencing factors, though two recent reviews help to distill some of the most popular ones. They identify surgery and internal medicine as the most desirable specialties and contend that lifestyle, work-life balance, and discipline interest were among the most influential factors cited.4 Graduating students’ decisions were contingent on lifestyle, workload, and clinical experiences, contrasting with younger peers who were more personally oriented (defined as focusing on “geography, self-confidence, and positive attitude toward patient population”).4 They suggest that societal orientation as well as prestige and income were also of particular salience in “non-occidental” (ie non-Western) countries and conclude that influencing factors differ in occidental (Western) contexts.4
This study addresses the determinants underpinning Qatar University medical students’ specialty choice by eliciting information about how, when and what factors are considered in our predominantly Arab-Islamic context. Identifying and understanding what factors can influence these choices can help academics and program administrators motivate students to explore specific fields, develop effective strategies to guide students through decisions surrounding medical career choices, and design curricula that promote and nurture a balanced interest in different specialties to ensure a robust future workforce capable of meeting the healthcare demands of the nation. Results from this study may also better inform policymakers’ decisions in anticipating unmet labor market needs within the local supply of physicians and to develop strategies to enhance the desirability of targeted specialties.
Methods
Context and Procedure
All students enrolled at the College of Medicine at Qatar University (QU) were invited to participate in an online study about residency choices in November 2022, toward the end of the Fall semester (ie Semester 1) of the 2022–23 academic year. An informed consent form and link to the survey were distributed via Qualtrics (Seattle, USA). The questionnaire remained open for six weeks with an email reminder sent at three weeks to boost participation. Study participation was voluntary, and informed consent was obtained before answering the questionnaire which took approximately 10 min to complete. All responses were anonymous, in line with Qatar University’s Institutional Review Board which granted approval for the study.
Measurements
The self-administered questionnaire comprised three sections: sociodemographic data, questions about specialty selection and their determinants. The survey was developed by five experts in the field of medical education and piloted on 10 medical students to ensure face and content validity. Students selected their residency preferences from an a priori defined list of specialties available in Qatar (Appendix 1). A list of 28 a priori defined determinants compiled by the research team were subsequently reclassified under the themes identified in Levaillant et al’s systematic review of occidental and non-occidental medical students’ choices to allow for useful comparison.4 Responses about factors influencing specialty selection were grouped under Levaillant’s themes: work-life balance, societal obligation, prestige and income, place of practice, specialty-related factors, and role models (see Appendix 2).
Data Analysis
Student selections were classified into three categories: surgical (if the student chose surgical only), non-surgical (if the student chose non-surgical only), and mixed (if the student selected a combination of surgical and non-surgical residency choices). Training year was also collapsed into two categories: preclerkship (year 1, 2, and 3) and clerkship (year 4, 5 and 6). Descriptive analyses were used to summarize the baseline characteristics of medical students participants. Categorical data were presented as numbers and percentages and continuous variables were summarized as mean and standard deviation or median and interquartile range. Chi-square or Fisher’s exact test was used to detect statistical differences between groups for categorical variables. In addition, a multinomial logistic regression was performed to explore the association between the independent variables and specialty selection. All analyses were carried out using Stata 17 software (StataCorp, College Station, USA). The level of significance was set at p < 0.05.
Results
All 358 students enrolled at the College of Medicine were invited to participate, of which 184 students responded, representing a response rate of 51%. There was good representation from all training levels: 41 students (22.3%) in each of their third and fourth years, 30 students (16.3% of respondents) in each of their first and second years, 29 (15.8%) in their sixth year, and 11 (6.0%) in their fifth year (Table 1). The mean age of respondents was 20 years. A majority were female (73.9%), Qatari (54.3%), unmarried (97.3%) and enrolled in a pre-clerkship year (55.0%). Most of our respondents reported high levels of parental education: 75.6% of respondents’ mothers had tertiary education (17.4% secondary, 7.1% primary), and 70.6% of fathers had tertiary education (26.1% secondary, 3.3% primary). There are significant differences between pre-clerkship and clerkship participants in their specialty choice: clerkship students tended to opt for non-surgical specialties (43.1%), while pre-clerkship students were more likely to select mixed specialties (48.8%) (p = 0.002) (Table 2).
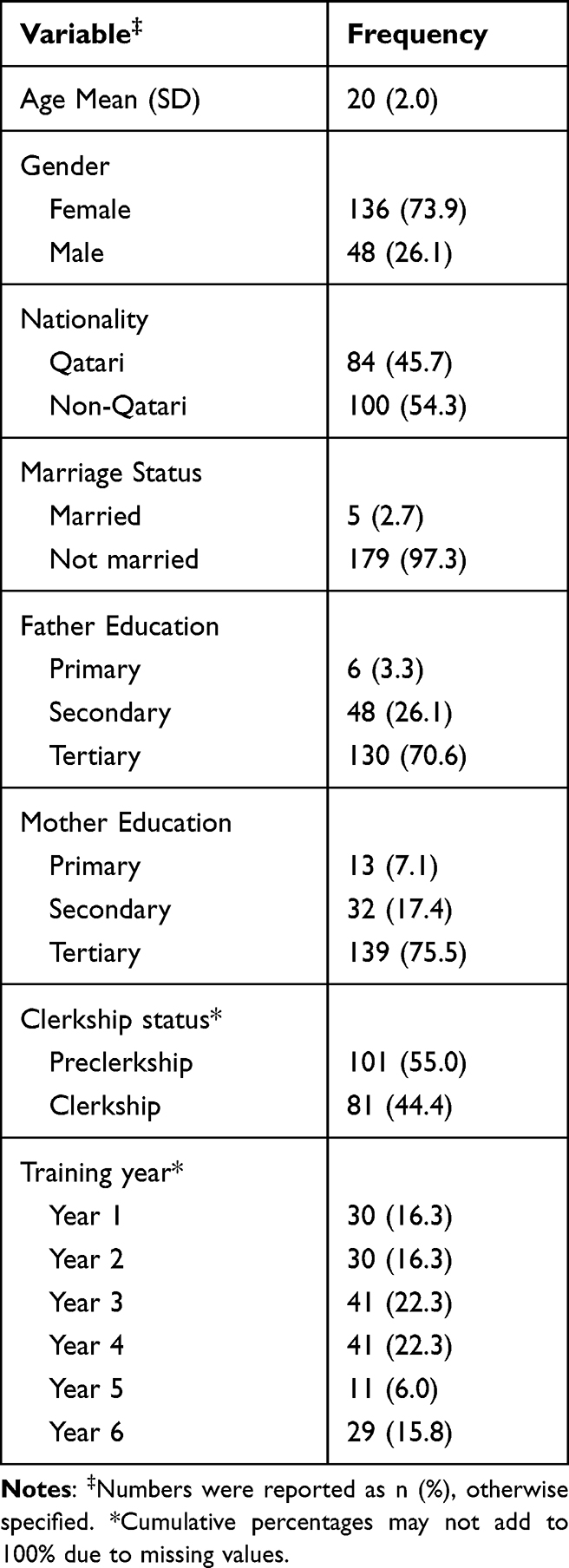 |
Table 1 Socio-Demographic Characteristics of Participants |
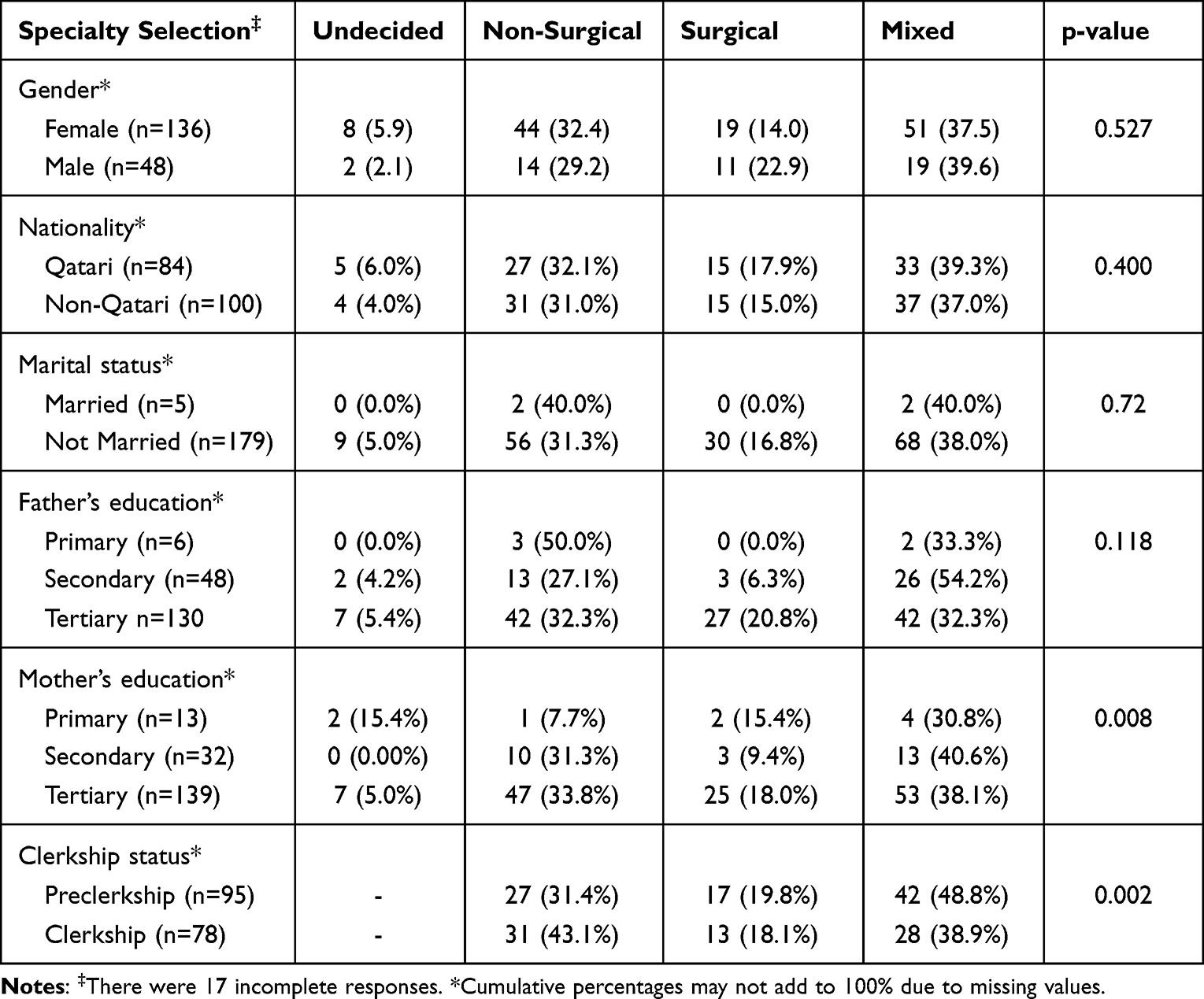 |
Table 2 Association Between Demographic Data and Specialty Selection |
Table 3 shows the association between specialty selection and determinants influencing medical students’ specialty choice. Prestige and income and role models seemed to be linked to the selection of a non-surgical specialty, representing approximately 44.8% and 41.7% of our respondents respectively (p = <0.001). On the other hand, mixed surgical/non-surgical specialties were preferred by students who emphasized the importance of work-life balance (47.5%), social obligations (48.4%), place of practice (42.4%), and factors related to the specialty itself (47.0%). Table 4 shows the residency choices of the respondents.
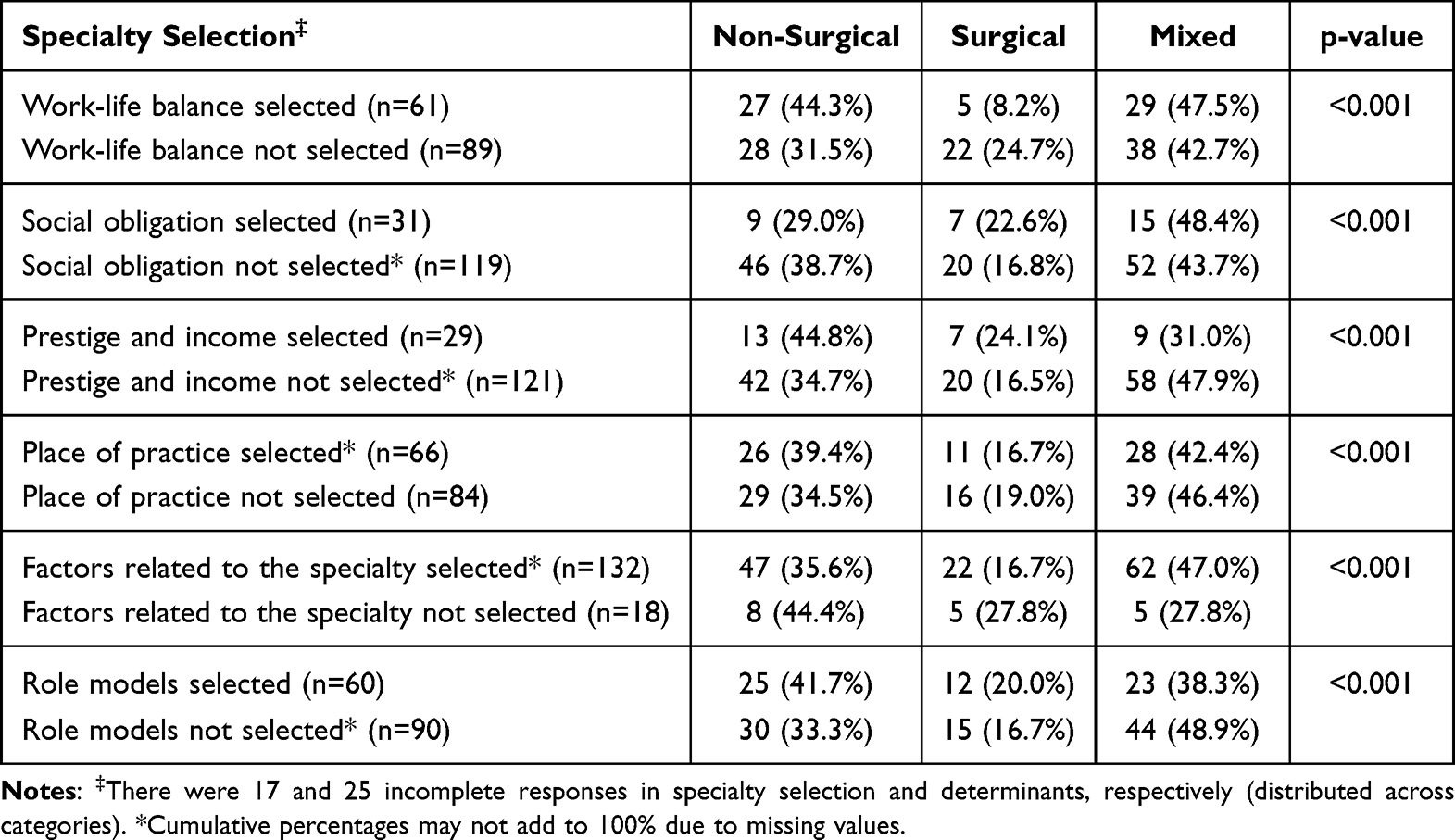 |
Table 3 Association Between Specialty Selection and Determinants Influencing Medical Students’ Specialty Choice |
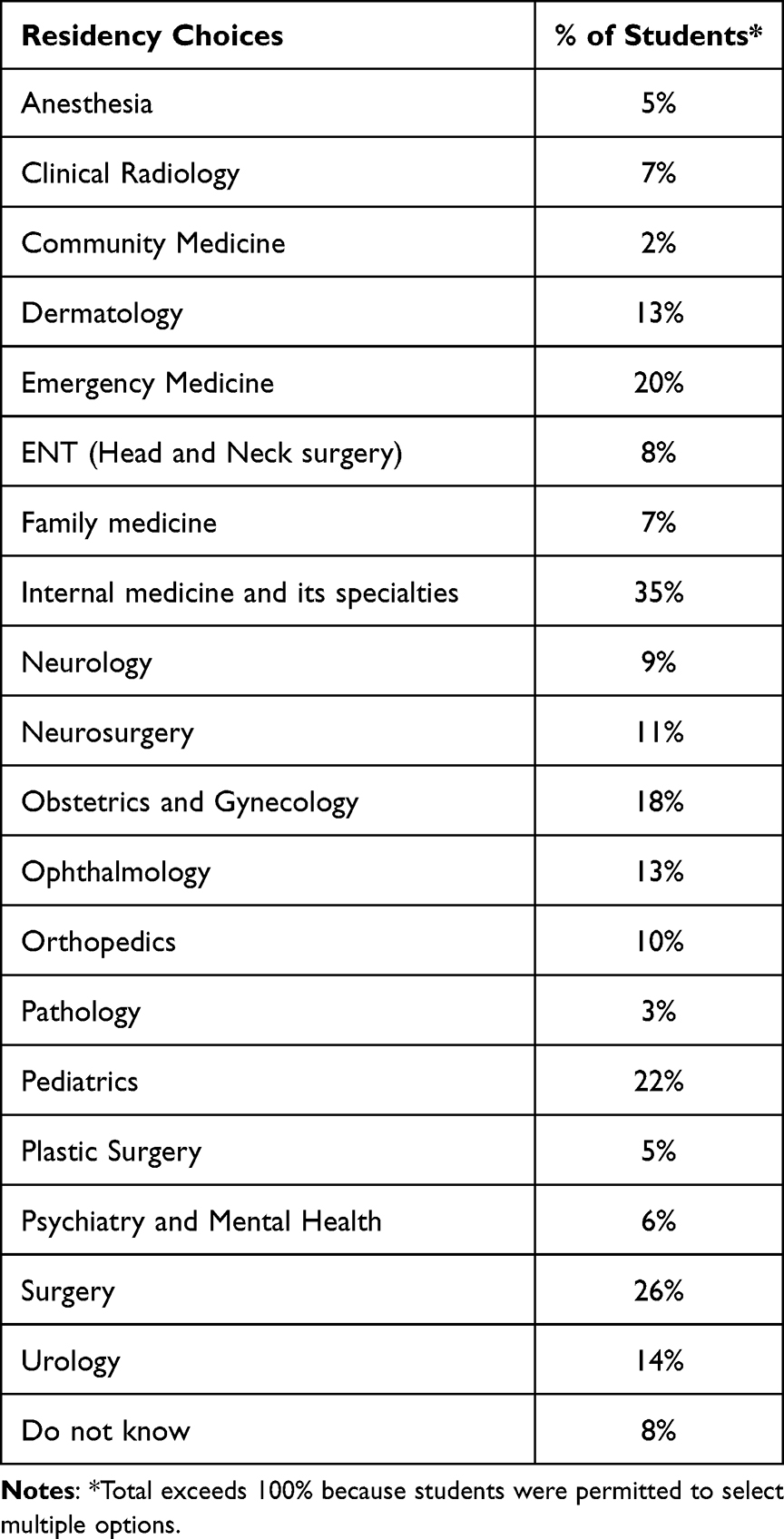 |
Table 4 Respondent Residency Choices |
Figure 1 shows career influences identified by students interested in each of the three categories of residency choices. For all types of residencies, specialty-related factors are consistently the most important (32.0–37.0% of students), and place of practice was consistently the third-most important (16.9–17.7%). The other types of influence – work-life balance, prestige and income, societal obligation, and role models and influencers – were important to different degrees among the different groups.
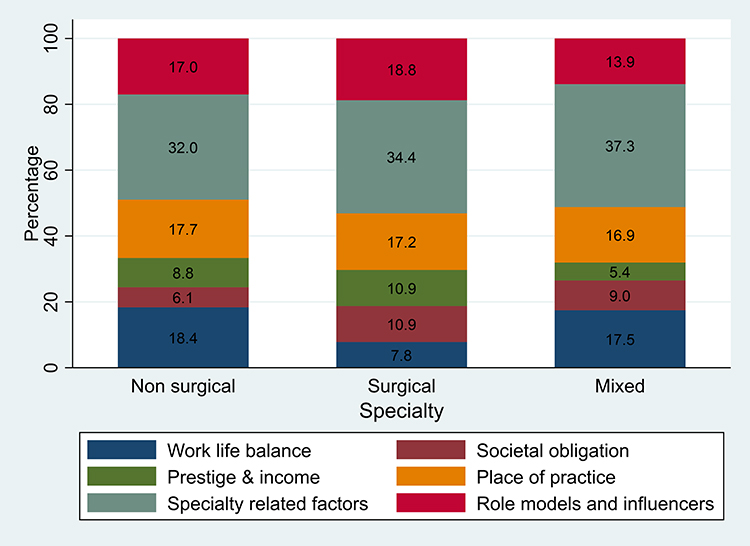 |
Figure 1 Determinants influencing medical students’ specialty choice. |
In Figure 2 we show the relative importance of career influences for male and female students; in Figure 3 this is further divided into the three groups of residency choices. Specialty-related factors remain the most often cited influence for all groups. Compared to female students, male students were overall more likely to cite role models and influencers, and females were more likely than male students to cite societal obligation as being important to them.
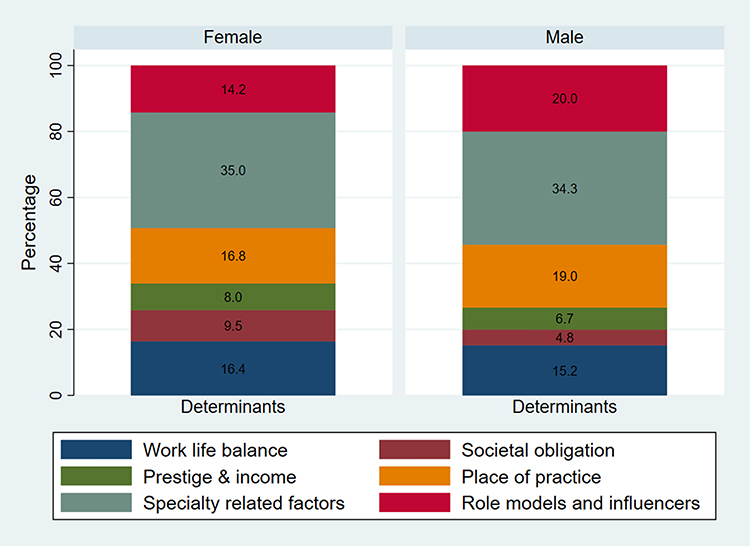 |
Figure 2 Determinants influencing female and male respondents. |
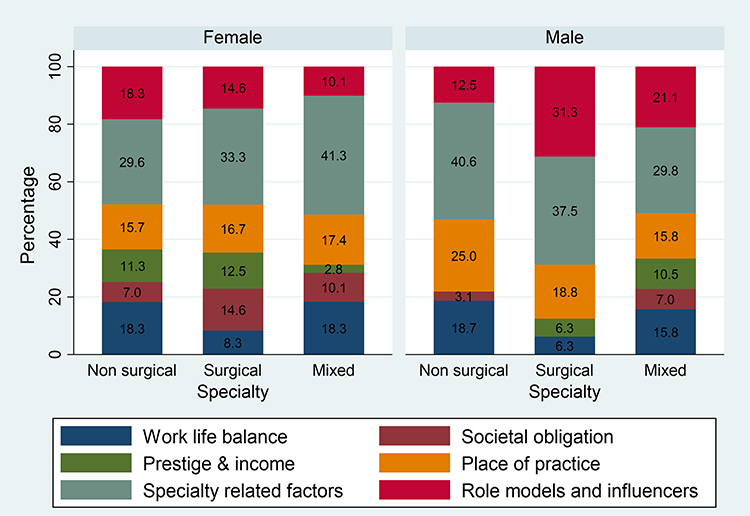 |
Figure 3 Determinants influencing medical students’ choice of specialization by specialty and gender. |
From Figure 4 we can see that the relative importance of some of these influences does appear to change over the course of the six-year medical program: specialty-related factors remain of primary importance to preclerkship and clerkship students, but place of practice is more important to clerkship students. Work-life balance is also more important to clerkship students, who are perhaps more familiar with the work demands that will shape their postgraduate life.
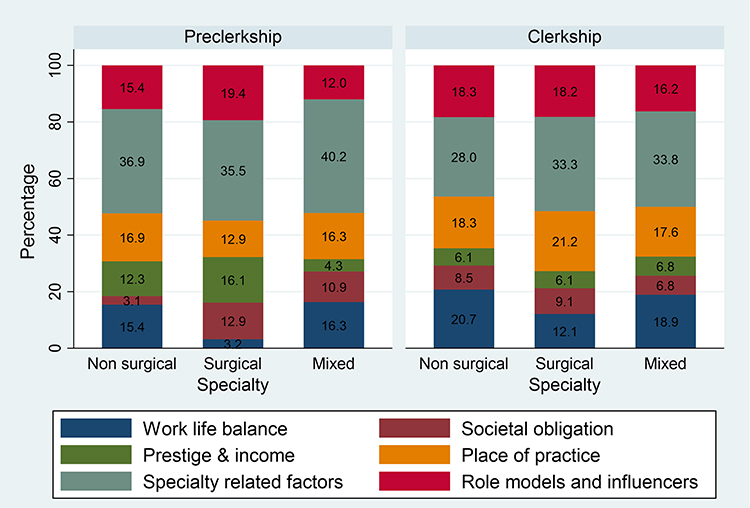 |
Figure 4 Determinants influencing medical students’ choice of specialization by specialty and clerkship status. |
Discussions
In line with studies from the region, our respondents cited specialty-specific factors as the number one factor in their residency decision.11,13,14 Other factors, of variable importance to different subgroups among our respondents, included work-life balance, role models, social obligation, place of practice, and prestige and income.
The most commonly cited determinant among our cohort was specialty-related factors. This corresponds to the literature from occidental and non-occidental countries.4,15 The residency-specific preferences of our cohort exhibit some similarities with medical student preferences from the United States and Canada. In all locations, internal medicine is selected by a large proportion of medical students (35% in our study, compared to 20% in the US16 and 18% in Canada) while pathology and community medicine are relatively unpopular choices.17 Pediatrics is very popular among our cohort (identified by 22% of students): it may be relevant that in this region, pediatrics is one of the specialties where both male and female practitioners can easily care for both male and female patients.
Family medicine in Qatar showed a similar popularity as in the USA, which is much less than in Canada: 7% at QU, compared to 8% in the United States and a striking 33% in Canada. The approach to health care practice in various jurisdictions seems directly linked to the popularity of family medicine. In Canada family physicians act as gatekeepers to healthcare. Family practice has less of a gatekeeper role in the United States, although family physicians may still play a key role in primary healthcare particularly in smaller and medium-sized communities.18 Qatar does not have a long-standing culture of family medicine. Before the establishment of the Primary Health Care Corporation in 2012, the Qatari culture of medical practice included direct patient access to subspecialty care. Qatar residents can also bypass the referral system offered through family medicine if they elect to visit one of the many private hospitals.
For both male and female respondents, work-life balance was only moderately important, with approximately 16% identifying it as an influence on their career choice. Results from a study of Kuwaiti medical students similarly found that only one fifth of students identify hours of work as an important determinant for career choice. Work-life balance is known to be important to North American and European medical trainees,19,20 particularly those of the millennial or Gen Z generations.21 In the USA, 82% of senior MD medical students identified work-life balance as important in selecting a residency program.16 Why is work-life balance less important to the students in our study? It is not a decreased emphasis on family life: the family has long constituted the primary support system in the Arab world.22 In Qatar, it is not unusual to live amongst one’s extended family wherein intergenerational kin (eg, grandparents, parents, aunts, uncles, and children) live under the same roof. The kinship support found in these domestic arrangements is in stark contrast to the more prevalent nuclear family arrangements found elsewhere where the physicians, particularly females, attend to domestic responsibilities.23,24 Another key difference between life as a physician in Qatar and life as a physician in North America and Europe is the ready availability of live-in domestic workers (eg. nannies) and drivers to help support working parents. In Qatar, it is routine to have this type of domestic support, while in North America and Europe, this may be financially prohibitive and is relatively uncommon. The prevalence of these family and domestic support arrangements in Qatar may alleviate the perceived burden of domestic responsibilities and reduce students’ concerns about work-life balance.
Consistent with earlier studies, our study participants do seem to have specialty preferences in mind upon entry to their medical studies.25–27 This is despite their young age, average age of 20 years, having started their six-year medical training program straight out of high school at age 18 unlike their American counterparts who start school on average at the age of 24.28 The relatively younger cohort of Qatar University medical students are largely unmarried, childfree, and supported financially by their families and the state. Alshahrani et al’s study demonstrated that lifestyle was significantly more important to interns as compared to medical students, indicating that as students age the realities of juggling the competing demands of work and family life become more important.6
International data show increasing “feminization” of the medical workforce, with a female to male medical student ratio of 48:5228 and 56:4417 in the US and Canada respectively. Middle Eastern and North African medical schools have an even more pronounced intake of female students: female to male ratios are 61:39 in Sudan, 64:36 in Jordan, and 57:43 in Kuwait,11,13,14 Saudi Arabian data reveal that while females account for more than half of medical school graduates, they constitute only a third of the current medical workforce.29,30 The female preponderance among our respondents is even more striking, with a 3:1 ratio of female to male students. In some countries, a lack of mentorship for female physicians and physicians-in-training has been reported;31,32 the preponderance of female medical students in Qatar could lead to a similar concern here.
In the survey, male and female respondents placed a different emphasis on three types of influences affecting their career preferences: role models, social obligation, and prestige and income. Male students were almost 50% more likely to cite role models and influencers as being important in their choice, whereas female students are twice as likely to say that social obligation is important to them (Figure 2). No males who selected a surgical specialty selected societal obligation as being relevant to their career choice, whereas females with a preference for surgery ranked it third in their list of considerations (Figure 3). As noted elsewhere, there appear to be fewer female role models than male role models currently in some locales;33 this is likely the case in Qatar. Same-sex mentorship can have a profound impact on the success of female medical/surgical trainees.34 The increasing feminization of the medical workforce in Qatar may expose a mentorship deficit over the next several years.
In two similar studies from Arab/Islamic countries in the region, social obligation was identified as an important factor in medical student career choice. To Sudanese medical students, being “helpful to the community” was the second most important specialty-selection influence,14 while a “lack of … this specialist in my country” was noted by almost a third of Kuwaiti students as being a reason they chose their specialty.11 In their systematic review of influences on medical student career choice, Levaillant et al show that in “occidental countries” (North America, European Union, Australia, New Zealand) medical students only infrequently identify societal orientation as being important in their career choice, where societal orientation is defined as willingness to provide an important service to the community.4 In “non-occidental countries” (ie everywhere else), social orientation is the third most important influence, behind only work-life balance and interest in the specialty itself. Our survey shows that for these students in (“non-occidental”) Qatar, societal obligation is of limited but real importance, and appears to be twice as important to female as to male students; the increased importance of societal obligation to women is also reported by Levaillant.4 Respondents in our survey described this influence as reflecting what “my country needs” and whether the specialty would “benefit my community”. For many students in this region, it seems social obligation is a significant consideration; this is in stark contrast to American medical students, for whom social obligation and related factors appear to have been completely omitted from a list of 57 factors influencing residency selection.16 This discrepancy may be due to an emphasis on group (eg. tribal or national) importance in Gulf and Gulf-adjacent Arab/Islamic populations, and a more individual-minded approach in American (or, more broadly, “occidental”) populations.35
Male and female respondents who chose either a surgical or non-surgical specialty emphasized prestige and income to different extents. Among male students who identified prestige and income as being relevant to their career choice, none chose a non-surgical specialty. Female students interested in surgical or non-surgical specialties were considerably more likely than male students to emphasize the importance of prestige and income; they were roughly equally likely to opt for a surgical and non-surgical career. Clearly from our study, males interested in prestige and income are more likely to choose a surgical than a non-surgical specialty. This is consistent with evidence from elsewhere that, at least for males, “students pursuing surgery…were more motivated by economics”.36 Interestingly, this did not appear to be the case for our female respondents. The reason for this discrepancy is not clear and warrants further investigation.
While specialty income is one of the factors that American medical students consider, it does not seem overall to be a decisive factor in residency choice,37 although it does seem to be becoming more important over time.38 Student debt also does not seem to be a significant determinant of American medical student career choice.39 Similarly, among our respondents, income is not a primary consideration for most students. Our respondents (average age 20 years) entered medical school as undergraduates, similar to medical students in the UK and the Middle Eastern region in general. In contrast, North American medical education is overwhelmingly postgraduate—American medical students start school on average at the age of 24.40 Qatar medical students are also supported financially by the state and most graduate with zero debt. These differences in age and financial support may lead to very different decision-making landscapes. Any comparison of occidental and non-occidental medical student residency choices should take into consideration these important contextual differences.
This study analyzes student preferences at a single institution in an affluent nation. Based in a predominantly Arabic and Islamic context, its students may have different personal and familial influences from students elsewhere. Focus groups probing specialty-specific decision-making would provide a more nuanced understanding of medical career choice in Qatar.
Conclusions
This study examines Qatar medical students’ career choices and motivations and provides some insight into the factors influencing these decisions. Specialty-related factors are the determinants which matter the most in the selection of residencies by medical students in Qatar. Other important determinants include role models, social obligation, place of practice, work life balance, and prestige and income. This study provides a baseline for future longitudinal and qualitative research exploring Qatar medical student residency preferences.
Disclosure
The authors report no conflict of interest.
References
1. Hutt R, Parsons D, Pearson R. The timing of and reasons for doctors’ career decisions. Health Bulletin. 1981;39(3):173–181.
2. Wright B, Scott I, Woloschuk W, Brenneis F. Career choice of new medical students at three Canadian universities: family medicine versus specialty medicine. CMAJ. 2004;170(13):1920–1924. doi:10.1503/cmaj.1031111
3. Zeldow P, Preston R, Daugherty S. The decision to enter a medical specialty: timing and stability. Med Educ. 1992;26(4):327–332. doi:10.1111/j.1365-2923.1992.tb00177.x
4. Levaillant M, Levaillant L, Lerolle N, Vallet B, Hamel-Broza J-F. Factors influencing medical students’ choice of specialization: a gender based systematic review. EClinicalMedicine. 2020;28:100589. doi:10.1016/j.eclinm.2020.100589
5. Bittaye M, Odukogbe A-TA, Nyan O, Jallow B, Omigbodun AO. Medical students’ choices of specialty in The Gambia: the need for career counseling. BMC Med Educ. 2012;12:1–9. doi:10.1186/1472-6920-12-72
6. Alshahrani M, Dhafery B, Al Mulhim M, Alkhadra F, Al Bagshi D, Bukhamsin N. Factors influencing Saudi medical students and interns’ choice of future specialty: a self-administered questionnaire. Adv Med Educ Pract. 2014;397–402. doi:10.2147/AMEP.S69152
7. Al-Ansari SS, Khafagy MA. Factors affecting the choice of health specialty by medical graduates. J Family Community Med. 2006;13(3):119. doi:10.4103/2230-8229.97541
8. Schmidt LE, Cooper CA, Guo WA. Factors influencing US medical students’ decision to pursue surgery. J Surg Res. 2016;203(1):64–74. doi:10.1016/j.jss.2016.03.054
9. Abdulrahman M, Makki M, Shaaban S, et al. Specialty preferences and motivating factors: a national survey on medical students from five UAE medical schools. Educ Health. 2016;29(3):231. doi:10.4103/1357-6283.204225
10. Khader Y, Al-Zoubi D, Amarin Z, et al. Factors affecting medical students in formulating their specialty preferences in Jordan. BMC Med Educ. 2008;8(1):1–7. doi:10.1186/1472-6920-8-32
11. Al-Fouzan R, Al-Ajlan S, Marwan Y, Al-Saleh M. Factors affecting future specialty choice among medical students in Kuwait. Med Educ Online. 2012;17(1):19587. doi:10.3402/meo.v17i0.19587
12. Alsubaie HM, Alsubaie KM, Alswat KA. Factors affecting the future medical specialty and training location selection. Saudi J Health Sci. 2017;6(3):163. doi:10.4103/sjhs.sjhs_35_17
13. Awadi S, Al Sharie S, Faiyoumi BA, E A, Hailat L, Al-Keder B. Factors affecting medical student’s decision in choosing a future career specialty: a cross-sectional study. Ann Med Surg. 2022;74:103305. doi:10.1016/j.amsu.2022.103305
14. Alawad AAMA, Khan WS, Abdelrazig YM, et al. Factors considered by undergraduate medical students when selecting specialty of their future careers. Pan Afr Med J. 2015;20(1). doi:10.11604/pamj.2015.20.102.4715
15. Murphy B The 11 factors that influence med student specialty choice. 2020.
16. National Resident Matching Program. Results and data: specialties matching service 2022 appointment year. Available from: https://www.nrmp.org/wp-content/uploads/2022/03/2022-SMS-Results-Data-FINAL.pdf.
17. Association CM. Canadian physician resources: 2012 basic facts. CMA(22 October 2012); 2012.
18. Green LA, Fryer GE
19. Gennissen L, Stegers-Jager K, van Exel J, Fluit L, De Graaf J, De Hoog M. Career orientations of medical students: a Q-methodology study. PLoS One. 2021;16(5):e0249092. doi:10.1371/journal.pone.0249092
20. Picton A. Work-life balance in medical students: self-care in a culture of self-sacrifice. BMC Med Educ. 2021;21(1):1–12. doi:10.1186/s12909-020-02434-5
21. Fernandez Nievas IF, Thaver D. Work–life balance: a different scale for doctors. Front Pediatr. 2015;3:115. doi:10.3389/fped.2015.00115
22. Abdul-Haq AK. The Arab Family: Formation, Function and Dysfunction. Caring for Arab Patients. CRC Press; 2018:77–88.
23. Frank E, Harvey L, Elon L. Family responsibilities and domestic activities of US women physicians. Arch Fam Med. 2000;9(2):134. doi:10.1001/archfami.9.2.134
24. Lorber J. Women Physicians: Careers, Status, and Power. Vol. 281. Tavistock Publications; 1984.
25. Budhathoki SS, Zwanikken PA, Pokharel PK, Scherpbier AJ. Factors influencing medical students’ motivation to practise in rural areas in low-income and middle-income countries: a systematic review. BMJ open. 2017;7(2):e013501. doi:10.1136/bmjopen-2016-013501
26. Cleland J, Johnston PW, French FH, Needham G. Associations between medical school and career preferences in year 1 medical students in Scotland. Med Educ. 2012;46(5):473–484. doi:10.1111/j.1365-2923.2012.04218.x
27. Svirko E, Goldacre MJ, Lambert T. Career choices of the United Kingdom medical graduates of 2005, 2008 and 2009: questionnaire surveys. Med Teach. 2013;35(5):365–375. doi:10.3109/0142159X.2012.746450
28. Colleges AAoM. 2018 Physician Specialty Data Report. Washington, DC, USA: American Association of Medical Colleges; 2018.
29. Ministry of Health. Statistical yearbook 1437H. Kingdom of Saudi Arabia; 2015. Available from https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/StatisticalBook‐1436.pdf.
30. Aldosari H. The Effect of Gender Norms on Women’s Health in Saudi Arabia. Washington, DC: Arab Gulf States Institute in Washington; 2017.
31. Steiner-Hofbauer V, Katz HW, Grundnig JS, Holzinger A. Female participation or “feminization” of medicine. Wiener Medizinische Wochenschrift. 2023;173(5–6):125–130. doi:10.1007/s10354-022-00961-y
32. Weigel KS, Kubik-Huch RA, Gebhard C. Women in radiology: why is the pipeline still leaking and how can we plug it? Acta Radiol. 2020;61(6):743–748. doi:10.1177/0284185119881723
33. Farkas AH, Bonifacino E, Turner R, Tilstra SA, Corbelli JA. Mentorship of women in academic medicine: a systematic review. J Gen Intern Med. 2019;34(7):1322–1329. doi:10.1007/s11606-019-04955-2
34. Lin G, Murase JE, Murrell DF, Godoy LDC, Grant-Kels JM. The impact of gender in mentor–mentee success: results from the women’s dermatologic society mentorship survey. Int J Women Dermatol. 2021;7(4):398–402. doi:10.1016/j.ijwd.2021.04.010
35. Hofstede G. Culture’s Consequences: International Differences in Work-Related Values. Vol. 5. Sage; 1984.
36. Ladha FA, Pettinato AM, Perrin AE. Medical student residency preferences and motivational factors: a longitudinal, single-institution perspective. BMC Med Educ. 2022;22(1):187. doi:10.1186/s12909-022-03244-7
37. Dorsey ER, Jarjoura D, Rutecki GW. Influence of controllable lifestyle on recent trends in specialty choice by US medical students. JAMA. 2003;290(9):1173–1178. doi:10.1001/jama.290.9.1173
38. Newton DA, Grayson MS, Thompson LF. The variable influence of lifestyle and income on medical students’ career specialty choices: data from two US medical schools, 1998–2004. Acad Med. 2005;80(9):809–814. doi:10.1097/00001888-200509000-00005
39. Kahn MJ, Markert RJ, Lopez FA, Specter S, Krane NK, Krane NK. Is medical student choice of a primary care residency influenced by debt? Medscape J Med. 2006;8(4):18.
40. AoAM C. Physician Specialty Data Report. Washington, DC: Association of American Medical Colleges; 2020.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.