")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Effects of Entry Grades on Students’ Academic Performance Under Homogeneous Educational Resources
Authors Huang N, Xiao Y, Chen W, Wang X
Received 28 October 2023
Accepted for publication 9 March 2024
Published 10 April 2024 Volume 2024:15 Pages 293—300
DOI https://doi.org/10.2147/AMEP.S444964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Naya Huang,1,* Yiying Xiao,2,* Wei Chen,1 Xin Wang1
1Department of Nephrology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China; Key Laboratory of Clinical Nephrology of the NHC (Sun Yat-Sen University) and Guangdong Provincial; Key Laboratory of Nephrology, Guangzhou, 510080, People’s Republic of China; 2School of Medicine, Sun Yat-Sen University, Shenzhen, Guangdong, 518170, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Chen; Xin Wang, Department of Nephrology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China; Key Laboratory of Clinical Nephrology of the NHC (Sun Yat-Sen University) and Guangdong Provincial; Key Laboratory of Nephrology, Guangzhou, 510080, People’s Republic of China, Tel +86-20-87766335, Email [email protected]; [email protected]
Background: A minor difference in college entrance examination scores can result in vastly different educational resources in China, so it has been debated whether it is the difference in the student population or the difference in educational resources that causes the difference in medical graduates. We aimed to evaluate the effects of entry grades on students’ academic performance under homogeneous educational resources.
Methods: Students in grade 2016 with 13-point difference in the average admission scores of 2 medicine schools in Sun Yat-sen University were educated in mixed classes and were taught with the same educators during the 5 years of undergraduate period. The grades, graduation, and postgraduate enrollment rates of the students were compared between the two campuses.
Results: The average admission scores for Shenzhen Campus (SZC) students are 13 points lower than those of Guangzhou North Campus (GZNC) (613 points vs 626 points). After 5 years of homogeneous education, comparing the GZNC students with the SZC students, there were no significant differences in the average total score (80.2 ± 4.6 vs 80.0 ± 5.6, P = 0.691), the average compulsory course (78.9 ± 3.4 vs 78.4 ± 6.1, P = 0.438), the average core course score (78.8 ± 7.4 vs 78.7 ± 5.0, P=0.860) and the average clerkship score (85.1 ± 7.2 vs 84.6 ± 2.7, P=0.275). However, the completion rate for SZC was higher than for GZNC (93.94% vs 86.27%, P=0.009). There was no statistical difference in postgraduate enrolment between the two institutions (P=0.758).
Conclusion: Given the same educational resources, more medical students with lower entrance scores completed their studies and achieved the same percentage of postgraduate acceptance. This finding suggests that a key component of improving the quality of medical higher education in China may be to further rationalize the allocation of high-quality educational resources, rather than to pursuing students with high entrance examination scores.
Key Messages: 1. Undergraduates from two medical schools with different average admission scores were educated with the same resources during the 5-year undergraduate period. After 5 years of homogeneous education, more students with lower entrance scores completed their studies and achieved the same percentage of postgraduate acceptance.
2. The key to improving educational quality is to optimize educational resources, not just to recruit high-scoring students.
Keywords: medical education, teaching quality, student quality, education sources
Introduction
The selection of students for higher education through entrance examinations is still the predominant method in China today.1 A difference of 10–20 points in college entrance examination scores will result in students being admitted to universities that differ significantly in educational resources. Although it has long been argued that educational resources determine the quality of education more than entrance exam scores, good educational resources always attract students with higher scores, so it is often difficult to define the difference in educational quality as the difference in student quality or the difference in educational resources.2,3 Compared with the means of improving the overall quality of educators and increasing the administrative support for education, attracting high-quality students has become the most convenient means for Chinese universities and colleges to improve the quality of education.4,5 Do higher admission scores lead to better educational outcomes though? Especially in medical education, it is more difficult to evaluate the quality of the educating due to the sociality of medicine, the complexity of the learning content, and the particularity of the organization and management of the education. Previous studies of the association of the “quality” of admitted students on education quality are based on subjective views or analogical analysis, and few studies are based on objective data.6 During the establishment of the Sun Yat-sen University School of Medicine (Shenzhen Campus, SZC), students from the SZC and the Sun Yat-sen University School of Medicine (Guangzhou North Campus, GZNC) participated in the same mixed classes throughout their time in medical school, completely eliminating the possible aggregation effect of the difference of educational resources on the quality of students and allowed us to analyze objectively the association of the limited quality difference of students on the quality of education. This study aims evaluate the effects of entry grades on students’ academic performance under homogeneous educational resources.
Methods
In this work, undergraduates in the 2016 entry-cohort, who majored in clinical medicine in SZC and GZNC, were included and followed up to July, 2021. There was a limited difference in the average admission score in Guangdong province (which occupied 50% of the students in 2016 entry cohort) between them. The average admission scores for SZC students were 13 points lower than those of GZNC (613 points vs 626 points). As the construction of SZC was not complete, those students would study in GZNC after admission, so it could be considered that they encountered a similar curriculum implementation and staff. Currently, students from both campuses had completed their undergraduate studies. Students’ curricular grades during the five-year undergraduate period were all collected.
Curriculum Context
The curriculum consists of public courses, basic specialized courses, core courses, clerkship courses, and clinical internship. Public courses include Medical Mathematics, Health Law, Medical Statistics, Preventive Medicine, Epidemiology, and Evidence-Based Medicine, College English, Medical Physics, Fundamentals of Computer Science, Physical Education. The basic specialized courses include Biology and Cell Biology, Basic Anatomy, Histology and Embryology, Physiology, Biochemistry and Molecular Biology, Medical Immunology, Medical Microbiology, Medical English, Pathology, Pharmacology, Pathophysiology, Clinical Anatomy, Medical Genetics, Human Parasitology, Molecular Medicine Skills, Experimental Physiology, Basic Chemistry, Medical Ethics, Diagnostics. Core courses included Internal Medicine Theory, Traditional Chinese Medicine, Pediatrics Theory, Medical Imaging, Clinical Nuclear Medicine, Medical Psychology, Surgery Theory, Obstetrics and Gynecology Theory, Neurology Theory, Infectious Disease Theory, Psychiatry Theory, Oncology Theory, Otorhinolaryngology Theory, Ophthalmology Theory, Dermatology and Venereology Theory, Clinical Skill Training. The clerkship courses focused on theoretical tutoring and clinical observation, included clerkships in internal medicine, surgery, pediatrics, obstetrics and gynecology, infectious diseases, psychiatry, oncology, otolaryngology, ophthalmology, dermatology and venereology, and neurology. The 48-week Clinical Internship was practical courses, it was set up to rotate in internal medicine, surgery, pediatrics, obstetrics and gynecology, dermatology, neurology, otolaryngology, infectious diseases, etc. All these curricular grades were collected to perform statistical analysis.
Among them, the average score of the total score was the average score of all the courses; the average score of compulsory courses was the average score of public courses, basic courses, and core courses; the average score of core courses was the average score of the above-mentioned core courses. The average score of the clerkship courses was the average score of all the clerkship courses; the average score of the internships was the average score of all the internship departments. The internship score was made up of a 30% rotation score, a 28% comprehensive examination score, and 42% comprehensive operation scores. In addition, clerkship courses and internships are uniformly classified as practical courses.
To compare the distribution of students’ grades, according to the average score, students’ grades were divided based on quartiles and classified into three groups.
- Excellent: ranking in top quarter of the average total score;
- Good: ranking in the middle two-quarters of the average total score;
- Qualified: ranking in the bottom quarter of the average total score.
Statistical Analysis
Continuous variables are summarized with the mean ± standard deviation. Categorical variables are summarized with numbers and percentages. The main comparisons made were between students from SZC and GZNC. The objective academic performance of students in the two cohorts was compared using the student t-test and the Wilcoxon rank sum test. The correlation between practical course grades and theoretical was assessed by Pearson correlation coefficient. A P<0.05 was considered statistically different. Analyses were with SPSS 13.0.
Results
Differences in Average Scores of Undergraduate Theoretical and Practical Courses Between Students from SZC and GZNC Under Same Educational Resources
A total of 165 students came from SZC and 415 from GZNC. The average admission scores for SZC students are 13 points lower than those of GZNC (613 points vs 626 points). After 5 years of homogeneous education, the statistical results are presented below. Compared with the GZNC students, there was no significant difference in the total score (80.2 ± 4.6 vs 80.0 ± 5.6, P = 0.691), basic specialized courses score (78.9 ± 3.4 vs 78.4 ± 6.1, P = 0.438), core course score (78.8 ± 7.4 vs 78.7 ± 5.0, P = 0.860) and the internship score (85.1 ± 7.2 vs 84.6 ± 2.7, P=0.275) (Table 1 and Figure 1). The average score for the 48-week clinical internships was significantly higher for GZNC students (78.3 ± 4.2 vs 82.1 ± 4.0, P<0.001). However, this might primarily be a subjective grade as the evaluation process depended greatly on teachers’ subjectivity.
 |
Table 1 Average Scores of the Five-Year Undergraduate Courses in Students of SZC and GZNC, Class of 2016 |
 |
Figure 1 Average scores of the five-year undergraduate courses in medical students of SZC and GZNC, Class of 2016. Abbreviations: SZC, Zhongshan University School of Medicine of Shenzhen Campus; GZNC, Zhongshan School of Medicine (Guangzhou North Campus). |
Differences in the Proportion of Excellent Students in Theoretical and Practical Courses Between Students from SZC and GZNC Under the Same Educational Resources
There was no significant difference in the proportion scoring excellent for total courses overall or for core courses between students from the two campuses (Table 2, 20.0% vs 21.4%, P=0.652. However, the excellent rate of basic specialized courses (26.8% vs 17.6%, P<0.001) and clinical internships (32.3% vs 10.9%, P<0.001) was higher in students in GZNC, while the proportion scoring excellent in clerkship courses was higher in SZC (44.2% vs 30.9%, P=0.008).
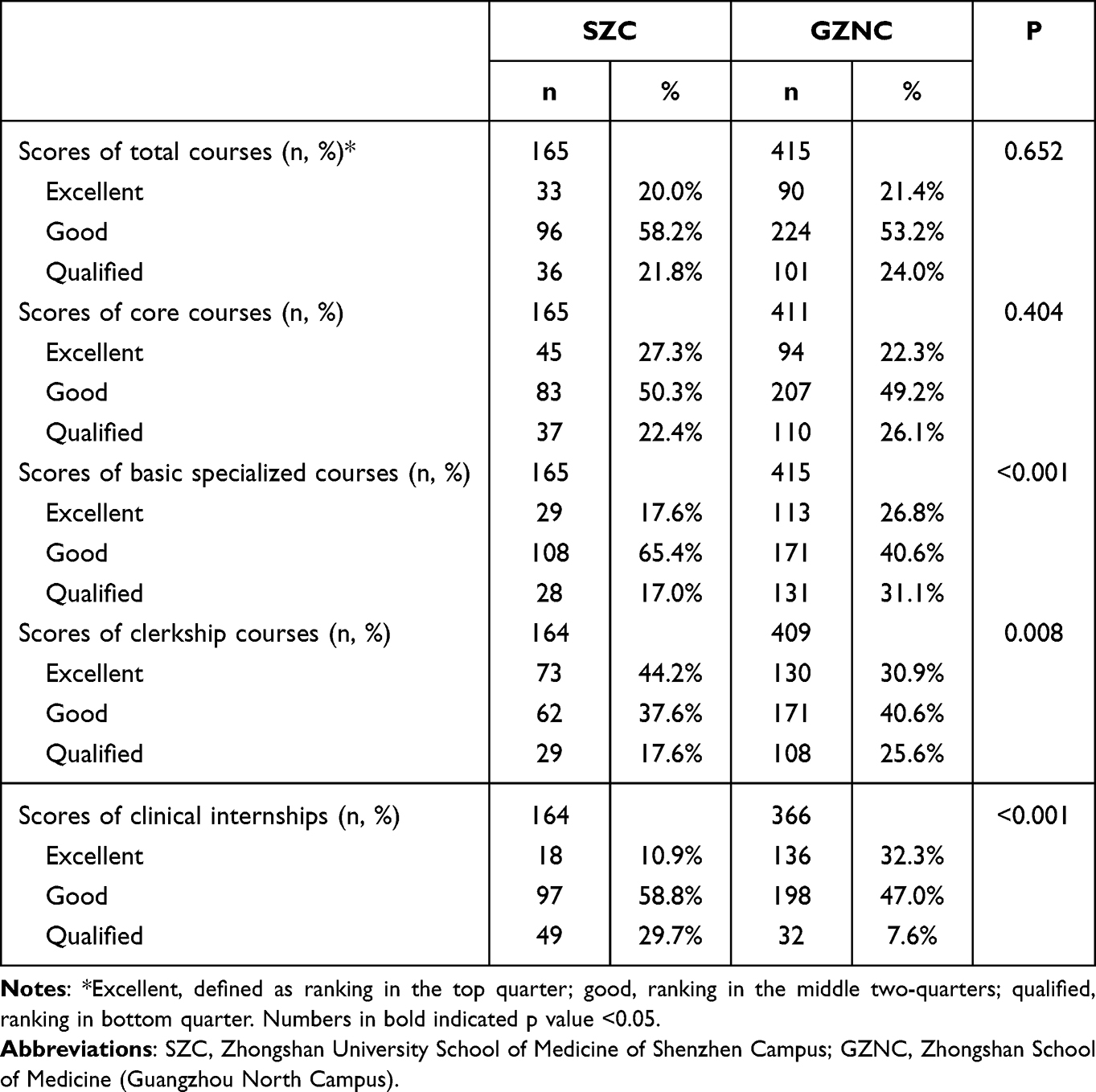 |
Table 2 Categories of Grades Between Medical Students in SZC and GZNC, Class of 2016 |
Comparison of SZC and GZNC Graduation and Post-Graduate Enrollment Rates
The SCZ graduation rate was higher than that of GZNC (93.94% vs 86.27%, P=0.009, Figure 2). The postgraduate enrollment rates for SZC and GZNC were 69.70% (115/165) and 70.84% (294/415), respectively (Figure 2). There are no statistical differences in postgraduate enrollment between the two cohorts (P=0.758).
 |
Figure 2 Graduation and post-graduate enrollment rates in medical students from SZC and GZNC, Class of 2016. (A and B) Were the graduation rates from SZC & GZNC; (C and D) Were the post-graduate enrollment rates from the SZC and GZNC. Abbreviations: SZC, Zhongshan University School of Medicine of Shenzhen Campus; GZNC, Zhongshan School of Medicine (Guangzhou North Campus). |
Relation Between Practical and Theoretical Marks
The results showed (Table 3) that the practical courses were positively correlated with the average scores of the total score, the basic specialized courses, and the core courses, either in all students combined or in students of SZC or GZNC separately. This therefore suggested that students with excellent scores in the theoretical courses also performed better in the practical courses.
 |
Table 3 The Correlation Between Practical Course Grades and Theoretical Course Grades Between Medical Students in SZC and GZNC, Class of 2016 |
Discussion
As mentioned above, although there was a significant difference of more than 10 points in the college admission scores of students from the two campuses, more medical students with lower entry scores completed their studies and achieved the same percentage of postgraduate acceptance. Our results show for the first time with objective data that better performance in medical school probably does not come from higher entrance scores. High entrance scores might even be considered a negative indicator of student success in higher medical education, as there are many high-scoring students who simply do not complete their studies.
The students in the two cohorts have the same educational tutoring resources and the evaluations are also carried out using the same tests and scoring system. Regarding theoretical courses, there was no statistical difference in the overall average score between the two cohorts and the respective average scores of the compulsory and professional courses that make up the overall average score except that GZNC students had better grades in clinical internships. To explore the underlying reason, we traced the specific process of this part of the examination and found that clinical performance evaluation, which accounts for a large proportion of internship results, was carried out and assessed independently in two hospitals with different assessment criteria. Since the evaluation of clinical performance was mainly a subjective evaluation by educators, the possibility of systematic deviation between hospitals cannot be ruled out.
Interestingly, GZNC students with higher entry scores had a greater dispersion of scores and lower completion rates at university level, suggesting that more of these “high scoring” students had failed examinations. The reasons for the marked divergence of students with higher entry scores during their university years are complex. In China, the high pressure of the college entrance exam and the high intensity of learning in high school often neglect students’ curiosity, sense of achievement and hope, so that some “high scorers” exhaust their enthusiasm for learning in high school and become bored with their studies when they enter university.7,8 At the same time, it is also possible that “high achievers” are those who are more comfortable with passive learning styles, who are more likely to gain an advantage in repeated examinations, but who are often unable to switch to active learning styles when they arrive at university, or who are unable to adapt to the environment of university life and develop psychological problems that prevent them from continuing their studies.9,10
Student quality, faculty education and qualifications and their academic characteristics, and administrative support were all believed to be the core components of high-quality higher education.5,11 Consistent with our study, there were studies that supported the core contents of high-quality educational resources being more dependent on faculty competence and experience than on student quality,12,13 and these determine the strength and depth of disciplinary and professional programs. Since the comprehensive quality of medicine integrates with tutoring and research in medical school educators, medical schools having higher requirements for faculties and high-quality resources are more difficult to obtain than general higher education.13,14 For medical education, improving educating quality lies not only in the ability and level of individual staff but also in the support and training of educating staff by schools and hospitals.15
Currently, the goal of our medical education has changed from cultivating applied medical professionals who will engage in medical services to cultivating research-oriented physicians with innovative ability, discovering problems in clinical work and the ability to solve problems.16,17 Higher medical education is not only the instillation of professional knowledge but also the ability and spirit of innovation in scientific research.18,19 Students who are good at memorizing are more likely to get good grades on examinations, but in practice, especially clinical practice and scientific research, these students may not perform as well as expected. Therefore, our study is not necessarily the most appropriate for using test scores during school, as well as the acceptance rate of graduate students, as a standard of educational quality. It may be more convincing to follow these students over a longer period, looking at their achievements 10 and 20 years later.
In addition, the evaluation of the quality of education is a very complicated process; it includes not only the academic performance of students but also the evaluation of moral development such as the ideals and beliefs of the students, social responsibilities, and behavior habits, as well as aesthetic literacy, labor practices, etc. It is difficult to quantify in the short term.17,18 However, the qualitative differences defined in our study were based solely on admissions performance; the conclusion of this study is limited to academic performance.
Conclusion
Given similar educational resources, more medical students with lower entrance scores completed their studies and achieved the same percentage of postgraduate acceptance. This finding suggests that a key component of improving the quality of medical higher education in China may be to rationalize further the allocation of high-quality educational resources rather than pursuing students with high entrance examination scores.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request and it’s not publicly available.
Ethics Approval and Consent to Participate
The Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University waived the requirement for informed consent for the study because the study did not involve any personal information. All methods were carried out in accordance with relevant guidelines and regulations for the present study and this study and it’s protocol was approved by the Guangdong Provincial Education Science Planning Office.
Consent for Publication
All authors gave their consent for publication.
Acknowledgments
We thank all colleagues at Sun Yat-sen University for their excellent data collection and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1. 2021 Guangdong Province Education planning project (Higher education special project:2021GXJK339). 2. 2023 University level teaching quality and teaching reform project (80000-12220011).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Arman A, Purwandaya B, Saefuddin A. The impact of quality of education and higher education on economic growth[j]. J Econ Educ. 2020;9(1):64–70. doi:10.15294/jeec.v9i1.36774
2. Kristina G, Howlett ZM. Meritocracy and its discontents: anxiety and the national college entrance exam in China. Asian J Soc Sci. 2021;51(2):2023129.
3. Zhang Z. Research on survey and development of high-quality education resources allocation from the perspective of fairness[J]. Adv Educ. 2015;05(04):69–75. doi:10.12677/AE.2015.54013
4. Skedsmo G, Huber SG. What does educational quality mean? Educ Assess Eval Account. 2021;33(4):587–589. doi:10.1007/s11092-021-09378-4
5. Dohms KP, Lettnin CDC, Mendes AR, et al. Affectivity of university teachers: personal, social and institutional aspects. Psychology. 2014;05(15):1783–1793. doi:10.4236/psych.2014.515185
6. Boatman A, Long BT. Does financial aid impact college student engagement? Res Higher Educ. 2016;57(6):653–681. doi:10.1007/s11162-015-9402-y
7. Ma P, He B, Pan W, et al. The influence of undergraduate’s mobile phone addiction on learning burnout: based on latent moderated structural equation. Psychology. 2020;11(06):966–979. doi:10.4236/psych.2020.116062
8. Zhang X, Liu B, Chen Z, Xu Y. An analysis of the factors affecting Chinese teenagers’ psychology of study-weary from the perspective of Satir’S Iceberg Theory. J Psychol Behav Stud. 2022;2(2):30–36. doi:10.32996/jpbs.2022.2.2.5
9. Shankland R, Kotsou I, Vallet F, et al. Burnout in university students: the mediating role of sense of coherence on the relationship between daily hassles and burnout. Higher Educ. 2019;78(1):91–113. doi:10.1007/s10734-018-0332-4
10. Asikainen H, Nieminen JH, Häsä J, et al. University students’ interest and burnout profiles and their relation to approaches to learning and achievement. Learn Individual Differences. 2022;93:102105. doi:10.1016/j.lindif.2021.102105
11. Yuan X. Construction of moral education evaluation model based on quality cultivation of college students. Sci Programm. 2022;2022:1–11.
12. Baitanayeva B, Aubakirova Z, Aitbembetova A, et al. Problems of improving the quality of education[J]. E3S Web Conf. 2020;159:9002. doi:10.1051/e3sconf/202015909002
13. Nikkhah M, Nikkhah A. Optimizing academic education: philosophies for creative quality lives. Creative Educ. 2011;02(05):458–460. doi:10.4236/ce.2011.25066
14. Altmiller G. Teaching quality improvement in prelicensure education. Nurse Educ. 2020;45(1):9–10. doi:10.1097/NNE.0000000000000772
15. Wong BM, Levinson W, Shojania KG. Quality improvement in medical education: current state and future directions. Med Educ. 2012;46(1):107–119. doi:10.1111/j.1365-2923.2011.04154.x
16. Syed RT, Singh D, Spicer D. Entrepreneurial higher education institutions: development of the research and future directions. High Educ Q. 2022. doi:10.1111/hequ.12379
17. Blouin D, Tekian A. Accreditation of medical education programs: moving from student outcomes to continuous quality improvement measures. Acad Med. 2018;93(3):377–383. doi:10.1097/ACM.0000000000001835
18. Concannon JP, Brown PL, Brown E. Prospective teachers’ perceptions of science theories: an Action Research Study. Creative Educ. 2013;04(01):82–88. doi:10.4236/ce.2013.41011
19. Chen CC, Wang NC, Tu YF, Lin HJ. Research trends from a decade (2011-2020) for information literacy in higher education: content and bibliometric mapping analysis. Proc Assoc Inf Sci Technol. 2021;58(1):48–59.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.