")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Growth Status of Full-Term Infants with Different Sizes for Gestational Age During the First Year of Life
Received 13 March 2024
Accepted for publication 4 July 2024
Published 8 August 2024 Volume 2024:15 Pages 265—272
DOI https://doi.org/10.2147/PHMT.S468778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Laurens Holmes, Jr
Zhuo-Ren Zhou, Yong Guo
Department of Health Care, Guangdong Women and Children Hospital, Guangzhou, 511400, People’s Republic of China
Correspondence: Yong Guo, Department of Health Care, Guangdong Women and Children Hospital, Guangzhou, 511400, People’s Republic of China, Tel +86 2039151521, Email [email protected]
Objective: This study aimed to assess the growth of full-term infants with different sizes at birth and examine catch-up and catch-down growth in their first year.
Methods: This retrospective population-based cohort study was based on the Guangdong Provincial Women and Children Health Information System. 194797 full-term singleton live births were extracted. Measurements for weight and length were taken at birth, 6 months, and 12 months. The size-for-gestational age was categorized as small (SGA, < 10th centile), appropriate (AGA, 10th-90th centiles), or large (LGA, > 90th centile) based on the international newborn size for gestational age and sex INTERGROWTH-21st standards. Catch-up and catch- down growth were defined as a change in standard deviation in z-score greater than 0.67 in the growth curves.
Results: Of the 194797 full-term singletons, the average gestational age was 39.28 ± 1.03 weeks, and the average weight of the newborns was 3205 ± 383 grams. 15632 infants were identified as SGA (8.0%) and 12756 were LGA (6.5%). At 1 year of age, catch-up growth in weight was observed in 63.0% of SGA infants, 29.5% of AGA infants, and 5.4% of LGA infants. Conversely, catch-down growth occurred in 3.3% of SGA infants, 17.8% of AGA infants, and 54.7% of LGA infants. The proportions of catch-up growth in length for SGA, AGA, and LGA infants within the first year were 31.4%, 22.5%, and 17.1%, respectively. Catch-up or catch-down growth predominantly occurred before 6 months of age. However, from 6 to 12 months, there was no significant variation in WAZ among children with different birth sizes.
Conclusion: In their first year of life, full-term singleton live births tend towards regression to the mean in their postnatal weight and length. The average delay in the growth of LGA is compensated by an increase in it of the SGA. Early monitoring and intervention are crucial for optimizing growth in infants with different birth sizes.
Keywords: growth status, infant, birth weight, catch-up growth
Introduction
Growth during the first year of life is a critical indicator of overall health and development in infants,1 reflecting the complex interplay between nutrition, genetics, hormones, and environmental factors. Early life, especially infancy, is a period of rapid brain and neurodevelopment and a critical window for rapid weight gain.2 Even faster weight gain or short-term growth decelerations during this crucial period may have long-term effects on organ development and function.3 The association between size for gestational age and subsequent growth status has been extensive research, as it provides valuable insights into the long-term health outcomes of infants.4–6 Both small for gestational age (SGA; birth weight < 10th percentile for gestational age) and large for gestational age (LGA; birth weight > 90th percentile) at birth are linked to increased neonatal morbidity and mortality risks.6–8 It has been observed that approximately 80% of infants classified as SGA show a notable positive growth response,9 contrasting with the potential occurrence of a distinct “catch-down growth ” in infants born LGA.10 The interaction between birth weight and early growth has significant implications, as it contributes to the subsequent risk of obesity and metabolic disease in later life.11,12 In addition, there is significant variation in rates of weight gain during the initial 1–2 years of life, and the growth status of infants can vary across different regions. Each region may have unique growth patterns influenced by various factors such as genetic predisposition, environmental conditions, cultural practices, and dietary habits.13–15 Currently, for infants with different birth weights, no consistent ideal growth curves target is well established. Moreover, there is a lack of comprehensive large-scale data specifically focused on the growth patterns of infants in the southern region of China. In this study, we aimed to examine infant catch-up and catch-down growth status using a population-based study. Systematic analyses of growth status were conducted between different birth weight groups and growth during the first year of life in southern China. It is hoped that by analyzing infant growth patterns through large-sample and real-world population cohorts, more clinical evidence can be accumulated for further child health intervention strategies.
Methods
Study Design and Data
A retrospective population-based cohort study was performed to assess the growth status in subjects born different sizes for gestational age during the first year of life. The data were obtained from the Guangdong Provincial Women and Children Health Information System, which collects information on mothers, newborns and regular health care from medical institutions in region of Guangdong, China.16 Maternal age, mode of delivery, gestational age at delivery, newborn sex, as well as weight and length measurements were extracted from the Guangdong Provincial Women and Children Health Information System. Measurements for weight and length were taken at birth, 6 months, and 12 months. The newborn birth weight and length were measured by obstetric medical staff. The weight and length at the ages of 6 and 12 months were measured by well-trained staff in community health centers. This study excluded multiple births, premature births (< 37 weeks of gestation age), and infants with congenital abnormalities. 194797 full-term singleton live births from January to December 2020 with complete information were included in our study.
Ethical Statement
Ethical approval for this study was obtained from the Medical Ethics Committee at Guangdong Women and Children Hospital (No. 202301234), which was conducted in accordance with the Declaration of Helsinki. The surveillance data utilized in this study were anonymized data sets, with all personally identifiable information removed. Consequently, the Medical Ethics Committee deemed the study exempt from the requirement of obtaining informed consent.
Definition of Birth Size for Gestational Age
The INTERGROWTH-21st gender-specific standards was used to define the categories of SGA, appropriate for gestational age (AGA), and LGA based on birthweight at each gestational week.17 SGA was defined as birthweight below the 10th percentile for gestational age, while AGA encompassed birthweight between the 10th and 90th percentiles. LGA was categorized as birthweight above the 90th percentile for boys and girls, respectively.
Definition of Growth Status
The main outcomes of infant growth in this study were assessed using the World Health Organization (WHO) international growth reference, specifically weight-for-age z-score (WAZ) and length-for-age z-score (LAZ) at 6 months and 12 months. Changes in WAZ and LAZ scores between birth and 6 months were calculated for weight and length (scores at 6 months minus scores at birth), and similarly, between birth and 12 months were calculated for weight and length (scores at 12 months minus scores at birth). The catch-up and catch-down growth were defined as a substantial change exceeding 0.67 standard deviation (SD) scores from birth to either 6 months or 1 year of age.18 A weight gain exceeding 0.67 SD scores was considered as clinically significant catch-up growth, as each 0.67 SD scores delineates the span of a percentile band on standard growth charts—from the second to ninth percentile, ninth to 25th percentile, 25th to 50th percentile, and so forth. Conversely, a reduction in weight SD scores by more than 0.67 SD scores indicated catch-down growth. This approach was adopted due to the fact that a change in weight SD score of 0.67 SD scores signifies the breadth of each percentile band on standard growth charts, highlighting substantial catch-up or catch-down growth.10,18–20 We considered underweight as a WAZ below −2 and stunting as a LAZ below −2.
Statistical Analysis
Anthropometric measurements and covariate data were stratified into SGA, AGA, and LGA groups. Group comparisons were conducted using analysis of variance (ANOVA) and χ2 tests for continuous and categorical variables, respectively. Continuous variables were presented as mean ± SD, while categorical variables were reported as percentages (%). Data analysis was performed using the SPSS statistical software package (V26, IBM Statistics, Chicago, IL, USA). P <0.05 was considered to be the threshold for statistical significance in analyses.
Results
The characteristics of the study subjects are presented in Table 1. Of the 194797 full-term singletons, the average gestational age was 39.28 ± 1.03 weeks, and the average weight of the newborns was 3205 ± 383 grams. 15632 (8.0%) were SGA and 12756 (6.5%) were LGA. Mothers of SGA infants had a relatively younger age compared to AGA and LGA mothers. The proportion of late-term infants (41–42 weeks) classified as SGA is relatively higher compared to LGA. At 1 year of age, 63.0% of SGA infants showed catch-up growth in weight, while 3.3% of SGA infants experienced catch-down growth. Among AGA infants, 29.5% showed catch-up growth in weight, and 17.8% experienced catch-down growth. Additionally, 5.4% of LGA infants exhibited catch-up growth in weight, while 54.7% experienced growth deceleration. The proportions of catch-up growth in length for SGA, AGA, and LGA infants within the first year were 31.4%, 22.5%, and 17.1%, respectively (Table 2).
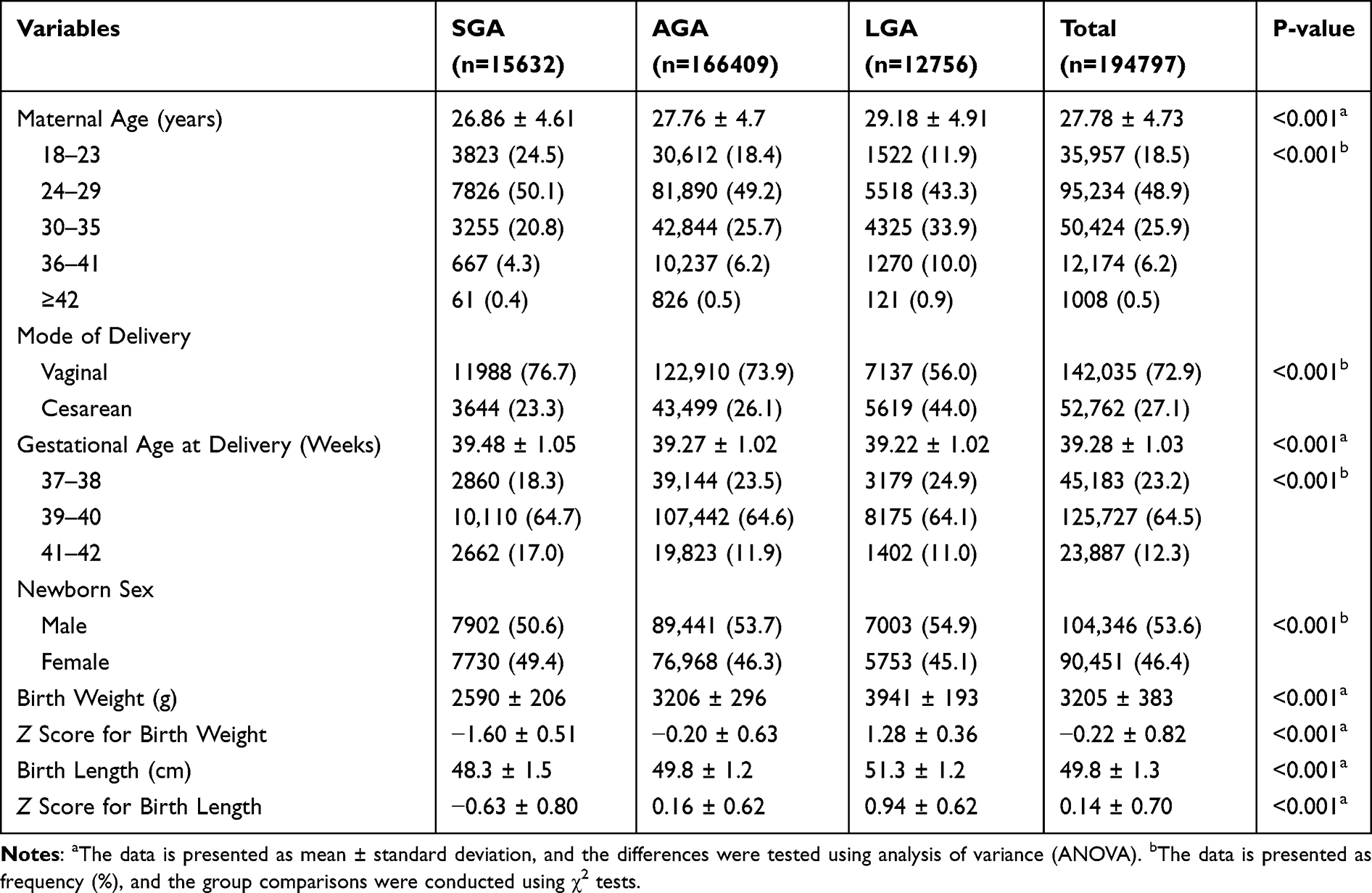 |
Table 1 The Characteristics of the Study Subjects |
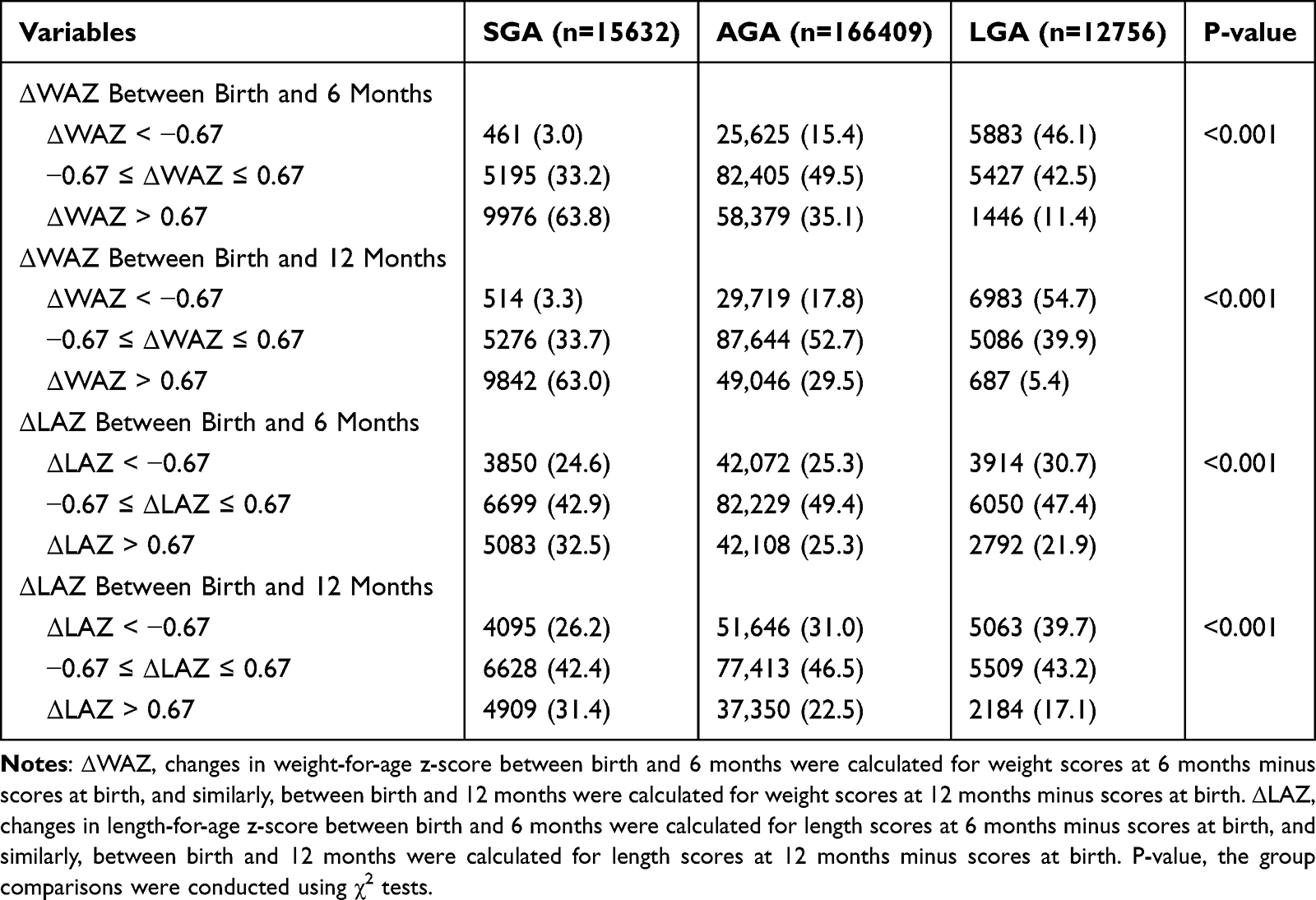 |
Table 2 Weight and Length Growth Status at 6 and 12 Months |
Figure 1 displays that SGA infants had lower WAZ than AGA and LGA infants at 6 and 12 months. SGA infants showed quick recovery, reaching a mean WAZ at 6 months. Regression to the mean may explain part of the SGA recovery, especially the notable increase in WAZ from birth to 6 months (ΔWAZ, 0.32 ± 1.01). However, from 6 to 12 months, there was no substantial variation in WAZ among children with different birth sizes (Figure 2). Among the three groups, the SGA group had the highest proportion of underweight at both 6 months (3.9% underweight) and 12 months of age (6.6% underweight), significantly higher than the AGA (0.8% at 6 months; 1.5% at 12 months) and LGA groups (0.2% at 6 months; 0.4% at 12 months). Similarly, regarding stunting, the SGA group had the highest proportion of stunting at both 6 months and 12 months of age (Table 3).
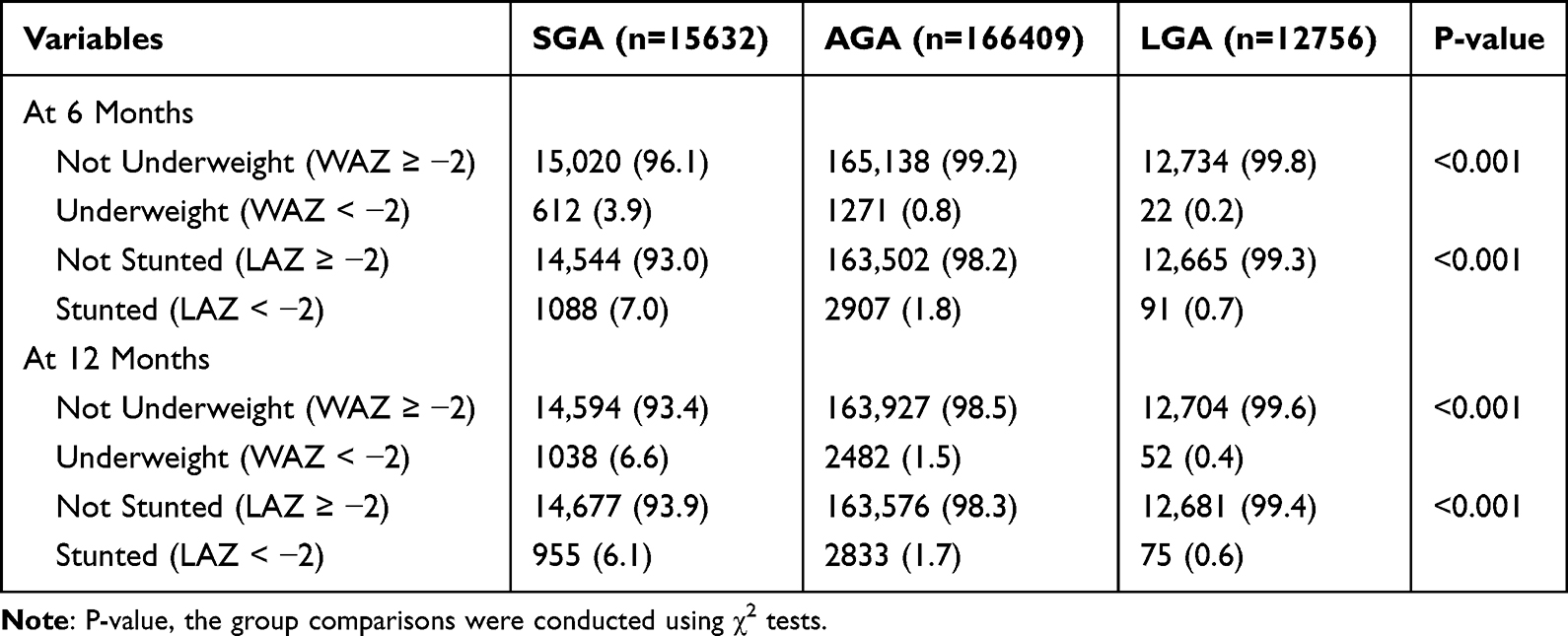 |
Table 3 The Prevalence of Underweight and Stunting During the First Year |
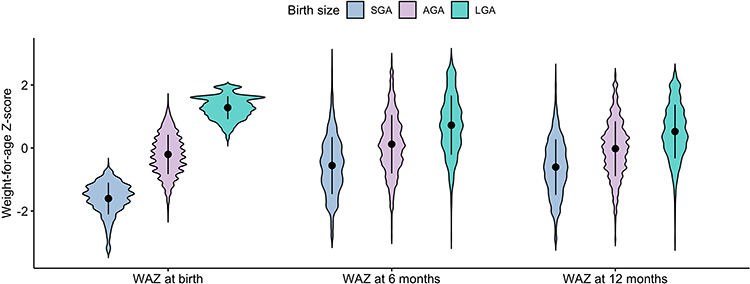 |
Figure 1 Weight for age z-score by birth size and age (SGA, small for gestational age; AGA, appropriate for gestational age; LGA, large for gestational age; WAZ, weight-for-age z-score). |
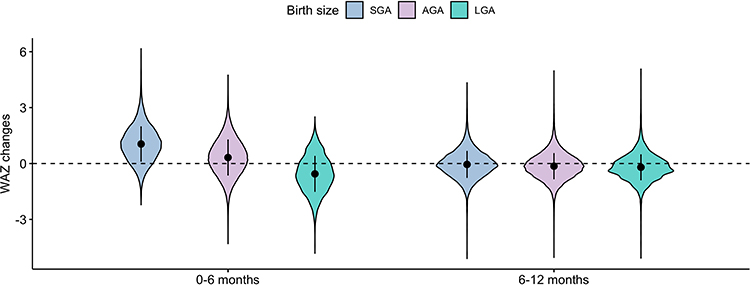 |
Figure 2 Weight for age z-score changes by birth size (SGA, small for gestational age; AGA, appropriate for gestational age; LGA, large for gestational age; WAZ, weight-for-age z-score). |
Discussion
Infants with different birth weights, often exhibit distinct growth patterns in early life.21 Understanding these growth dynamics is crucial for identifying potential risk factors and implementing appropriate interventions. In this study, we explored the growth patterns of SGA, AGA, and LGA infants within the first year of life and investigated the occurrence of catch-up and deceleration growth.
In line with previous studies using the INTERGROWTH-21st birth weight standards, we observed an SGA prevalence of 8.0% and an LGA prevalence of 6.5% among full-term singleton infants. These findings are similar with research conducted in China, employing the INTERGROWTH-21st birth weight standards, which reported comparable proportions for SGA and LGA classifications.22,23 Moreover, we observed that mothers of SGA infants tended to be younger compared to AGA and LGA mothers, suggesting a potential association between maternal age and the risk of SGA infants. Maternal age is a crucial factor influencing pregnancy outcomes, particularly among extreme age groups, such as young and older mothers, where this association may involve multiple factors.24–26 Young mothers might lack adequate nutritional knowledge or be unable to access the necessary nutrients due to economic or social reasons, potentially leading to fetal growth restriction. Additionally, young mothers might be more susceptible to adverse lifestyle influences, such as unhealthy diets and smoking, which are known risk factors for SGA. Socioeconomic factors also play a role; young mothers may have less access to high-quality medical care and support.27
Regarding growth patterns, Osamu et al examined current evidence regarding the association between early rapid growth and the risk of future obesity and cardiometabolic issues, focusing on the distinct implications of accelerated weight gain in infancy and early childhood.28 They suggest the importance of monitoring childhood growth patterns, particularly in the early stages before 1 year of age, as it may be linked to future obesity trends. We found that at 1 year of age, a substantial proportion of SGA infants (63.0%) showed catch-up growth in weight, indicating a recovery from their initial growth restriction. However, a small proportion of SGA infants (3.3%) experienced catch-down growth, suggesting persistent growth impairment. The definitions of early catch-up and catch-down growth remain variability, often determined by percentile or SD scores to identify significant growth changes.12 These definitions span age intervals from infancy to young adulthood, with the most pronounced variations in growth velocity typically observed within the initial year of life. In studies related to obesity, rapid growth is commonly defined as a WAZ change exceeding 0.67 SD between two different childhood ages.18 Our research according to this methodology, the results consistent with prior studies. Notably, up to 90% of SGA children experience catch-up growth by age 2, while catch-down growth is observed in 29–81% of LGA children.29,30 Among preterm infants, about 80% of late preterm and SGA infants showed catch-up growth in weight at 6 months of corrected age.31 Additionally, our study revealed that a significant proportion of LGA infants (54.7%) experienced growth deceleration. This suggests that despite their initial larger birth weight, these infants exhibited a trajectory towards returning to a normalization process. It is worth noting that a certain proportion of LGA infants (5.4%) showed accelerated growth. This finding raises concerns regarding the long-term implications of this subgroup of LGA infants. Numerous studies have established a link between excessive growth and long-term health outcomes.11,12 Consistent with previous studies,32,33 the observation of catch-up or catch-down growth occurring primarily before 6 months of age suggests a critical period for intervention to support optimal growth. Analyzing the prevalence of underweight and stunting, we found that the SGA group had the highest proportion of infants who were underweight and stunted at both 6 months and 12 months of age. This indicates that these infants may face challenges in achieving appropriate growth. Identifying the higher prevalence of underweight and stunting in the SGA group highlights the importance of addressing their specific nutritional needs and providing appropriate support for optimal growth. Healthcare professionals and caregivers should closely monitor the growth and development of SGA infants, ensuring that they receive adequate nutrition and interventions to promote catch-up growth and minimize the long-term effects of underweight and stunting.
Although there have been numerous studies on the relationship between birth weight and child growth patterns, our study further confirmed the significant differences in growth status within the first year of life among infants with different birth sizes. The strengths of our study are that it includes a large sample size and employs a longitudinal design. However, our study still has a few limitations that should be acknowledged. Firstly, the generalizability of the findings may be limited due to the specific characteristics of the sample population. Our study is the regional focus on the southern region of China. This geographical restriction may affect the generalizability of our findings to other regions or populations with different characteristics. Secondly, our retrospective study primarily focused on the growth status and characteristics of SGA, AGA and LGA infants, but information regarding exclusive breastfeeding and the economic status of the parents was not collected in our database. As a result, the control of variables was limited, and there were some confounding factors that could not be effectively controlled. Another limitation is the relatively short follow-up duration of only 1 year. Longer-term follow-up is necessary to assess the persistence of growth patterns and potential associated health outcomes, such as metabolic disorders or cognitive development.
Conclusions
In conclusion, our study provides valuable insights into the growth status of infants with different birth sizes in southern China. SGA infants primarily exhibit catch-up growth, predominantly occurring before 6 months of age. AGA infants maintain stable growth patterns throughout the first year of life, while more than half of LGA infants show catch-down growth. These findings emphasize the importance of early monitoring and intervention to support optimal growth in infants with different birth sizes.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Funding
This work was supported in part by the Medical Scientific Research Foundations of Guangdong Province, China [A2021125], Guangzhou Municipal Science and Technology Bureau [202102080278], and the Clinical Research Project of Guangdong Women and Children Hospital [310103-1637].
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Langley-Evans SC. Nutrition in early life and the programming of adult disease: a review. J Hum Nutr Diet. 2015;28(Suppl 1):1–14. doi:10.1111/jhn.12212
2. Miguel PM, Pereira LO, Silveira PP, Meaney MJ. Early environmental influences on the development of children’s brain structure and function. Dev Med Child Neurol. 2019;61(10):1127–1133. doi:10.1111/dmcn.14182
3. Silva CCV, El Marroun H, Sammallahti S, et al. Patterns of fetal and infant growth and brain morphology at age 10 years. JAMA Network Open. 2021;4(12):e2138214. doi:10.1001/jamanetworkopen.2021.38214
4. Langley-Evans SC, McMullen S. Developmental origins of adult disease. Med Princ Pract. 2010;19(2):87–98. doi:10.1159/000273066
5. Remacle C, Bieswal F, Bol V, Reusens B. Developmental programming of adult obesity and cardiovascular disease in rodents by maternal nutrition imbalance. Am J Clin Nutr. 2011;94(6 Suppl):1846S–52S. doi:10.3945/ajcn.110.001651
6. Calcaterra V, Cena H, Verduci E, Bosetti A, Pelizzo G, Zuccotti GV. Nutritional Surveillance for the best start in life promoting health for neonates, infants and children. Nutrients. 2020;12(11):3386.
7. Liu C, Wang K, Huang G, et al. Association of small-for-gestational-age status with mortality and morbidity in very preterm Chinese infants. J Matern Fetal Neonatal Med. 2023;36(2):2258257. doi:10.1080/14767058.2023.2258257
8. Chauhan SP, Rice MM, Grobman WA, et al. Neonatal morbidity of small- and large-for-gestational-age neonates born at term in uncomplicated pregnancies. Obstet Gynecol. 2017;130(3):511–519. doi:10.1097/AOG.0000000000002199
9. Karlberg J, Albertsson-Wikland K. Growth in full-term small-for-gestational-age infants: from birth to final height. Pediatr Res. 1995;38(5):733–739. doi:10.1203/00006450-199511000-00017
10. Taal HR, Vd Heijden AJ, Steegers EA, Hofman A, Jaddoe VW. Small and large size for gestational age at birth, infant growth, and childhood overweight. Obesity. 2013;21(6):1261–1268. doi:10.1002/oby.20116
11. Gatjens I, Fedde S, Schmidt SCE, et al. Relationship between birth weight, early growth rate, and body composition in 5- to 7-year-old children. Obes Facts. 2022;15(4):519–527. doi:10.1159/000522509
12. Nordman H, Jaaskelainen J, Voutilainen R. Birth size as a determinant of cardiometabolic risk factors in children. Horm Res Paediatr. 2020;93(3):144–153. doi:10.1159/000509932
13. Imdad A, Yakoob MY, Bhutta ZA. Impact of maternal education about complementary feeding and provision of complementary foods on child growth in developing countries. BMC Public Health. 2011;11(Suppl 3):S25. doi:10.1186/1471-2458-11-S3-S25
14. Alderman H, Nguyen PH, Tran LM, Menon P. Trends and geographic variability in gender inequalities in child mortality and stunting in India, 2006-2016. Matern Child Nutr. 2021;17(3):e13179. doi:10.1111/mcn.13179
15. Wehby GL, Lopez-Camelo JS. Maternal education gradients in infant health in four south American countries. Matern Child Health J. 2017;21(11):2122–2131. doi:10.1007/s10995-017-2327-7
16. Xu T, Miao H, Chen Y, Luo L, Guo P, Zhu Y. Association of interpregnancy interval with adverse birth outcomes. JAMA Network Open. 2022;5(6):e2216658. doi:10.1001/jamanetworkopen.2022.16658
17. Villar J, Cheikh Ismail L, Victora CG, et al. International standards for newborn weight, length, and head circumference by gestational age and sex: the newborn cross-sectional study of the INTERGROWTH-21st project. Lancet. 2014;384(9946):857–868. doi:10.1016/S0140-6736(14)60932-6
18. Ong KK, Ahmed ML, Emmett PM, Preece MA, Dunger DB. Association between postnatal catch-up growth and obesity in childhood: prospective cohort study. BMJ. 2000;320(7240):967–971. doi:10.1136/bmj.320.7240.967
19. Batista RF, Silva AA, Barbieri MA, Simoes VM, Bettiol H. Factors associated with height catch-up and catch-down growth among schoolchildren. PLoS One. 2012;7(3):e32903. doi:10.1371/journal.pone.0032903
20. Ay L, Van Houten VA, Steegers EA, et al. Fetal and postnatal growth and body composition at 6 months of age. J Clin Endocrinol Metab. 2009;94(6):2023–2030. doi:10.1210/jc.2008-2045
21. Ouyang F, Wang X, Wells JC, Wang X, Shen L, Zhang J. The associations of birthweight for gestational age status with its differential 0-2 year growth trajectory and blood pressure at two years of age in Chinese boys and girls. Nutrients. 2023;15(4):979. doi:10.3390/nu15040979
22. Zhang YQ, Li H, Zong XN, Wu HH. Comparison of updated birth weight, length and head circumference charts by gestational age in China with the INTERGROWTH-21st NCSS charts: a population-based study. World J Pediatr. 2023;19(1):96–105. doi:10.1007/s12519-022-00631-4
23. Wang X, Hui LL, Cole TJ, Nelson EAS, Lam HS. Fitness of INTERGROWTH-21st birth weight standards for Chinese-ethnicity babies. Arch Dis Child Fetal Neonatal Ed. 2023;108(5):517–522. doi:10.1136/archdischild-2022-325066
24. Cao J, Xu W, Liu Y, et al. Trends in maternal age and the relationship between advanced age and adverse pregnancy outcomes: a population-based register study in Wuhan, China, 2010-2017. Public Health. 2022;206:8–14. doi:10.1016/j.puhe.2022.02.015
25. Costantine MM, Tita ATN, Mele L, et al. The association between infant birth weight, head circumference, and neurodevelopmental outcomes. Am J Perinatol. 2024;41(S 01):e1313–e23. doi:10.1055/s-0043-1761920
26. Li J, Yan J, Jiang W. The role of maternal age on adverse pregnancy outcomes among primiparous women with singleton birth: a retrospective cohort study in urban areas of China. J Matern Fetal Neonatal Med. 2023;36(2):2250894. doi:10.1080/14767058.2023.2250894
27. Semrau KEA, Mokhtar RR, Manji K, et al. Facility-based care for moderately low birthweight infants in India, Malawi, and Tanzania. PLOS Glob Public Health. 2023;3(4):e0001789. doi:10.1371/journal.pgph.0001789
28. Arisaka O, Ichikawa G, Koyama S, Sairenchi T. Childhood obesity: rapid weight gain in early childhood and subsequent cardiometabolic risk. Clin Pediatr Endocrinol. 2020;29(4):135–142. doi:10.1297/cpe.29.135
29. Ong KK. Catch-up growth in small for gestational age babies: good or bad? Curr Opin Endocrinol Diabetes Obes. 2007;14(1):30–34. doi:10.1097/MED.0b013e328013da6c
30. Clayton PE, Cianfarani S, Czernichow P, Johannsson G, Rapaport R, Rogol A. Management of the child born small for gestational age through to adulthood: a consensus statement of the International societies of pediatric endocrinology and the growth hormone research society. J Clin Endocrinol Metab. 2007;92(3):804–810. doi:10.1210/jc.2006-2017
31. Vizzari G, Morniroli D, Tiraferri V, et al. Postnatal growth of small for gestational age late preterm infants: determinants of catch-up growth. Pediatr Res. 2023;94(1):365–370. doi:10.1038/s41390-022-02402-3
32. Karlberg JP, Albertsson-Wikland K, Kwan EY, Lam BC, Low LC. The timing of early postnatal catch-up growth in normal, full-term infants born short for gestational age. Horm Res. 1997;48(Suppl 1):17–24. doi:10.1159/000191279
33. Ahmad N, Sutan R, Tamil AM, Hajib N. Growth patterns and nutritional status of small for gestational age infants in Malaysia during the first year of life. Child Health Nurs Res. 2021;27(4):317–327. doi:10.4094/chnr.2021.27.4.317
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.