")
Back to Journals » Medical Devices: Evidence and Research » Volume 17
Quantifying Patient Capabilities and Setting the Stage for Future Development: Insights from a Sensor-Augmented Simulated Use Study with Pen Injectors
Authors Lange J , Schneider AE, Jordi C
Received 14 May 2024
Accepted for publication 24 July 2024
Published 31 July 2024 Volume 2024:17 Pages 271—283
DOI https://doi.org/10.2147/MDER.S478141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jakob Lange, Andreas E Schneider, Christoph Jordi
Ypsomed AG, Burgdorf, Switzerland
Correspondence: Jakob Lange, Email [email protected]
Background: While formative and summative usability testing is essential to confirm safe and effective product use, it may not be sufficient to comprehensively understand user capabilities and limitations in device interactions. Therefore, this research aims to quantify user handling forces for different device handling steps of pen injectors through sensor-augmented simulated use studies.
Research Design and methods: The study involved 46 participants who were divided into two groups: a healthy control group and a group of users with dexterity impairments. All participants were instructed to perform simulated handling steps using non-functional dummy devices equipped with force and torque sensors. Each handling step was performed twice: first at what participants considered a comfortable force level and then at their maximum force. The study then analyzed force data to investigate the impact of user characteristics and device geometry on force exertion during the different handling steps.
Results: The study demonstrates differences in the perceived comfortable and maximum force levels between the control and patient groups. These force levels decrease slightly with the user’s age and level of dexterity impairment. Furthermore, the forces applied by the users are dependent on the geometry of the device and the holding pattern.
Conclusion: The results highlight the significance of sensor-augmented simulated use studies as a tool for providing quantitative insights into users’ ability to exert force while handling self-injection devices. These data offer comprehensive insights that inform the definition of performance requirements and specifications for injection device design, thereby supporting the advancement of future self-injection devices.
Plain Language Summary: This study explores how people interact with pen injectors; devices commonly used for self-injections. Traditional usability tests are vital for ensuring safe product use, but they may not fully capture users’ capabilities and limitations. To address this gap, the research measures the forces exerted by users during different handling steps of pen injectors through a simulated use study with sensors.
Forty-five participants, including a healthy control group and individuals with dexterity impairments, engaged in handling non-functional dummy devices with force and torque sensors. Each participant performed handling steps twice, first at a comfortable force level and then at their maximum force. The study analyzed force data to understand how user characteristics and device geometry affect force exertion.
Results revealed differences in force levels between control and patient groups, with applied force levels decreasing slightly with age and dexterity impairment. The study emphasized the impact of device geometry and holding patterns on applied forces. Overall, the findings show the usefulness of sensor-augmented simulated use studies in quantifying users’ force exertion, providing insights for designing future self-injection devices.
Keywords: subcutaneous drug delivery, pen injector, simulated use, handling force, user capability, force sensor, torque sensor, user impairment
Introduction
Injection devices for the subcutaneous self-administration of therapeutic agents undergo rigorous formative and summative human factors testing to ensure safe and effective product use.1–5 Device manufacturers prioritize patient safety and involve users early in the design and development to achieve regulatory approval and ensure successful market access.6–8 Usability work has provided valuable insights into the user experience, acceptability, and preferences of various self-injection devices, ranging from cartridge-based pens that deliver multiple doses9–11 and autoinjectors to administer a single-dose bolus12,13 to on-body devices that enable large-volume injections.14,15
While usability work has traditionally focused on success rates and use errors,16,17 it has largely overlooked the capabilities and limitations of users that shape contextual user-device interactions. However, for three reasons, it is essential to have a more comprehensive understanding of users’ situational engagement with self-injection devices in general, and the handling forces required for each use step in particular. Firstly, optimal handling forces contribute to patient comfort during device use, making it easier for patients to become familiar with and adopt new, emerging therapies and adhere to prescribed treatment regimens.18–23 Previous research has consistently shown that device usability positively impacts treatment preferences and outcomes.24–26 Secondly, appropriate handling forces improve the accessibility of emerging self-care treatment options to a diverse user population.27 This aspect is essential in the current era of self-injection device platforms.2,11,12 The industry is adopting pre-engineered technologies to serve multiple target patient populations, including those with varying levels of strength and dexterity.28 Inappropriate handling forces can lead to use-related errors and jeopardize patient safety.17,27 Thirdly, meeting the stringent regulatory standards for self-injection devices is critical to obtain regulatory approval and a prerequisite for successful market adoption.29,30
Researchers have recently started studying the situational actions and use-related forces involved in patients’ interaction with autoinjector technology.27,31 These efforts provide a more nuanced understanding of the drug self-administration process. For instance, researchers have integrated motion and force sensors directly into autoinjector devices and accessories to analyse user behaviour for each handling step.31 Although this approach provides a wealth of quantitative insights, it can interfere with device handling by limiting the freedom of movement of the actuated device during normal handling. Schneider et al have addressed this shortcoming by using non-functional autoinjector prototypes with different predefined discrete force levels to assess the patient’s ability to remove the protective needle cap from an autoinjector.27 The approach described allows for a realistic handling sequence but does not provide continuous force data beyond the predefined force levels. Another approach that has been used involves adding force sensors to an injection pad, suitable for studying the patient’s ability to press the autoinjector device against the skin. However, this approach remains silent on all other user actions and interactions with the device during self-injection.32
Thus, our understanding of the handling forces encountered and applied during each step of self-injection device use is incomplete. The industry would benefit from detailed force data for different user groups, considering patient-specific characteristics such as hand strength and dexterity. This study aims to fill this gap by using a sensor-augmented approach to study the handling steps necessary for injecting with a pen device. Participants performed simulated handling using different device dummies equipped with force and torque sensors to obtain quantitative force data on users’ ability to perform the cap removal, dose setting, and injection steps. The study included a control group and a group of impaired experimental users who performed each usage step with what they considered to be comfortable and maximum force levels. The data was then analyzed to describe how user characteristics influenced their ability to apply force during the different handling steps. This information is crucial for defining user requirements and determining comfortable and maximally tolerable force levels.
Methods
Participants
Participants were recruited through an online patient panel in May 2020 and August 2020. Eligible individuals were identified through a screening questionnaire and their actual level of impairment as well as hand strength was then determined as part of the study. The study included an experimental group of lay users with reduced hand strength due to age and disease and a control group without dexterity impairments. Aged female participants were included in the experimental group as this user category is known to have reduced hand strength compared to younger and male users33 Table 1 shows the screening criteria and group composition. Participants were compensated with USD 150 for their participation.
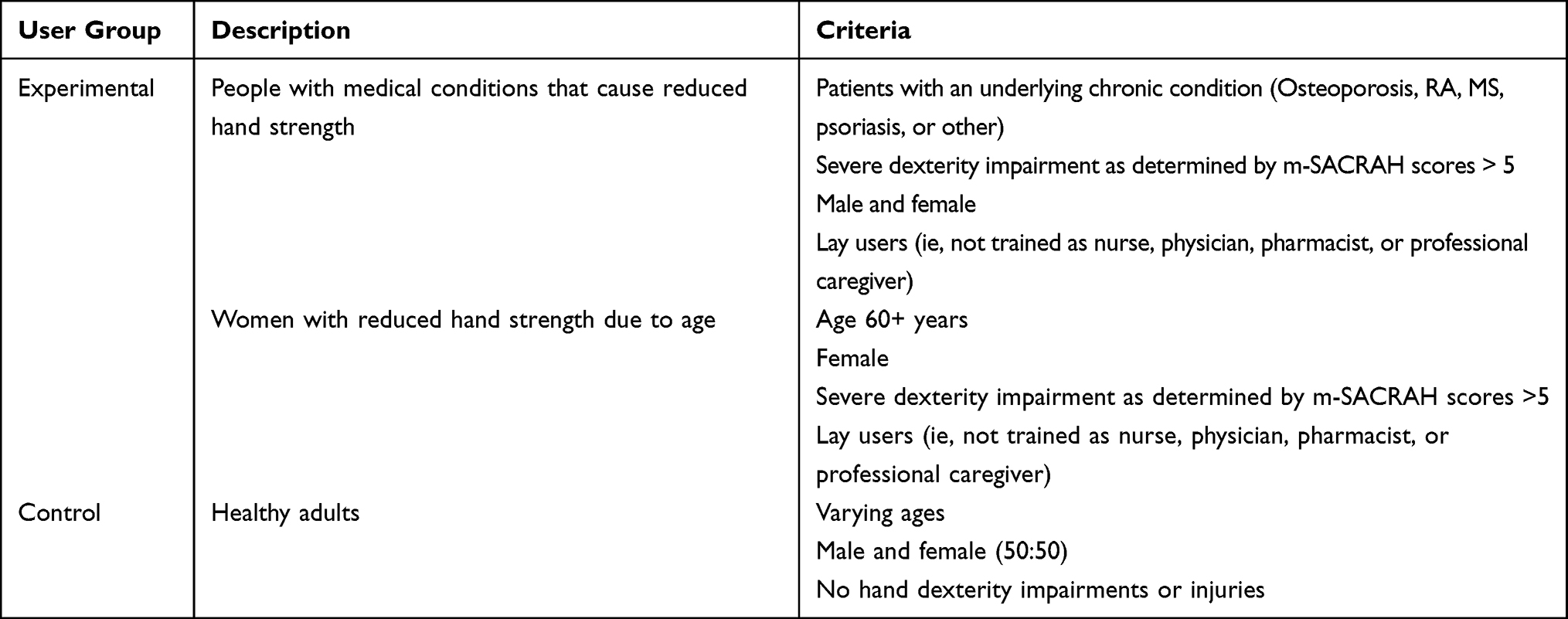 |
Table 1 Screening Criteria and Participant Group Description |
A total of 46 participants were included in the study. 15 participants with an average age of 33 years were recruited for the control group. Participants in the control group had no manual dexterity impairments. The older participants of the experimental group consisted of 15 participants with an average age of 65 years, while the patient group consisted of 16 participants with an average age of 55 years. Most of the participants in the experimental group had some chronic condition that resulted in manual dexterity impairment, and 2/3 of them had a moderate to severe level of impairment. Impairment was assessed using an abbreviated version of the M-SACRAH (Modified and shortened Score for the Assessment and Quantification of Chronic Rheumatoid Affections of the Hands) questionnaire. The abbreviated version had only 10 questions, leaving out the two ones associated with pain, and was assessed on a scale from 1–10. Results were grouped into the three categories; “Low” with scores 1.0–2.9, “Moderate” with scores 3.0–4.9 and “Severe” with scores 5.0–10.0.34 Table 2 presents the demographics and health status of the participants.
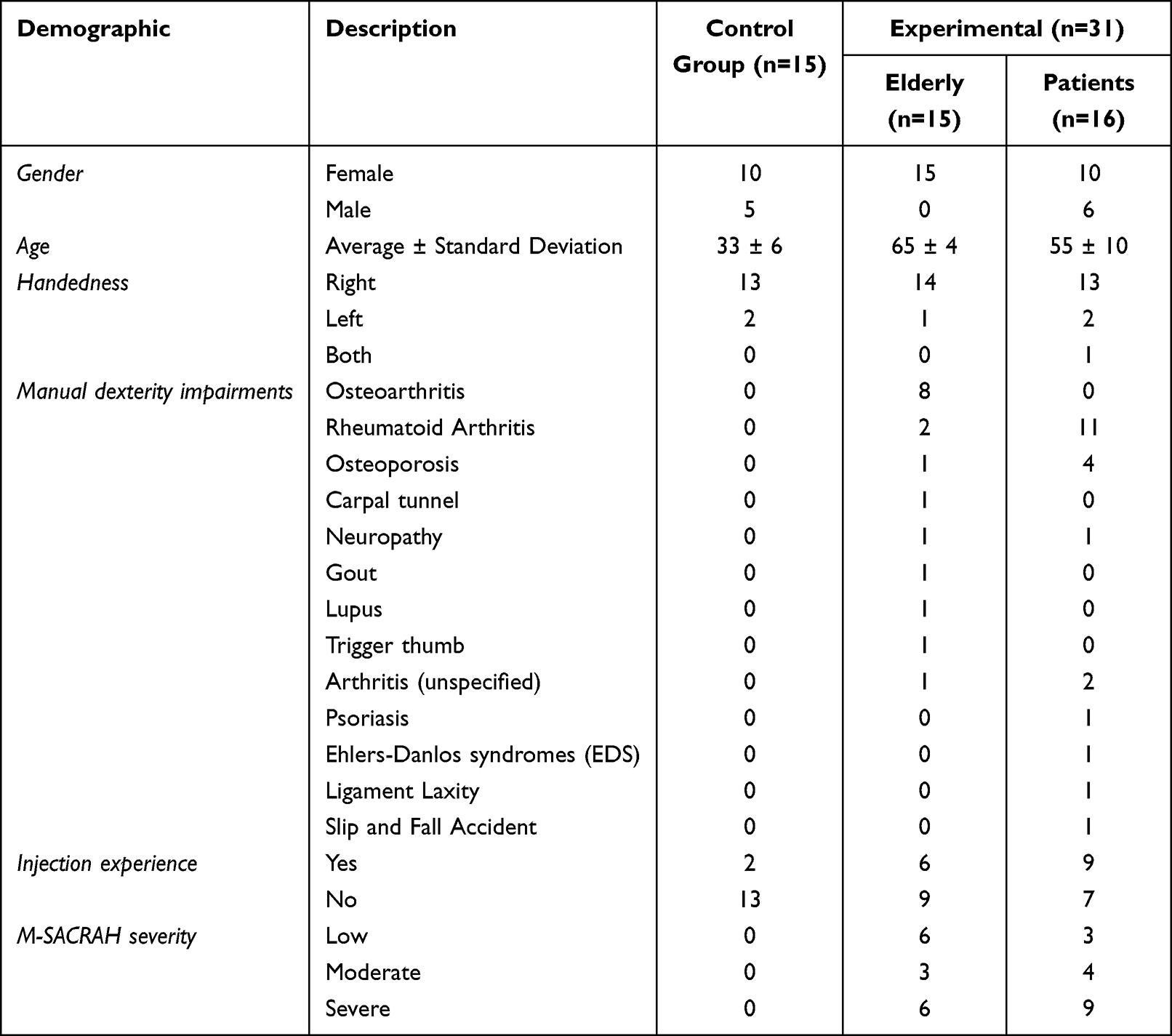 |
Table 2 Participant Demographics and Health Status |
Materials
The study was conducted using sensor-equipped device dummies. The device dummies were constructed to represent a manual pre-filled insulin-type pen injector, ie, a variable dial-and-dose pen intended for multiple injections from the same 3-mL cartridge, using parts of the UnoPen (Ypsomed AG, Burgdorf, Switzerland). This approach, combining real device parts, dummies, and sensors, was chosen because it has the advantage of allowing relatively realistic handling while providing continuous force data during use. It is important to note, however, that the force sensors allow very limited travel or amplitude during handling, which represents a significant difference compared to real device handling. Figure 1 shows the handling steps and the corresponding device dummies and parts used in the study. A Futek LCM-100 25 lbs loadcell with a cap dummy was used to measure the pull-of force for cap removal as shown in Figure 1 Step 1. To assess torque for dose selection, a Futek TAT-200 100 in-oz torque sensor was used with the rear end of an UnoPen (cf. Figure 1, Step 2). A Futek LLB-130 50 lbs loadcell attached to a complete UnoPen device captured compression force during simulated injection (shown as Step 3 in Figure 1). All sensors were connected to a data acquisition computer via a USB-520 signal processor. All force data was collected using the Futek SENSIT software.
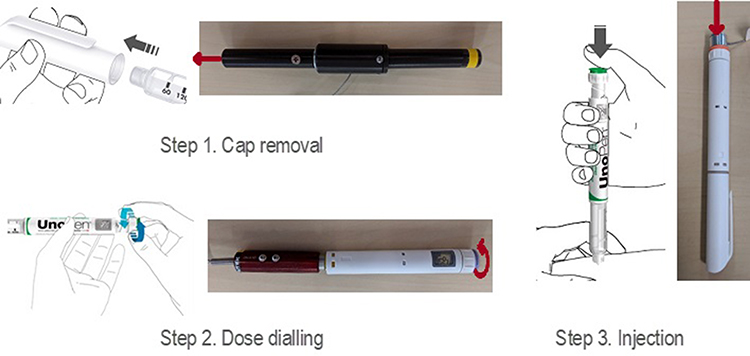 |
Figure 1 Illustration of handling steps and non-functional dummy devices with force and torque sensors used in the study. |
Hand strength was evaluated by measuring grip and pinch strength using standard equipment. A Saehan Hand Dynamometer SH5001, Saehan Corporation, South Korea, was used for grip strength, and a set of baseline mechanical pinch gauges from Fabrication Enterprises, USA, was used for pinch strength.
Procedure
The handling study followed standard protocols and procedures based on single site visits. The study was conducted in a simulated home environment. The study room had a one-way mirror on one wall that allowed observers (eg, data collectors) on the other side of the mirror to observe and listen to the study sessions. This study was conducted during the COVID-19 pandemic. Therefore, the moderator and the participant wore masks throughout the study. First, each participant’s demographic and health information, including any impairments, was collected, and baseline hand strength was measured with two measures of maximum pinch and grip strength. Trained staff then instructed participants to use the self-injection pen dummies and sensors by direct demonstration. Each participant was instructed to apply first a force they considered comfortable (“Apply the amount of force you would be comfortable with when performing the task”) and then their maximum (“Apply the maximum/highest amount of force you can use to perform the action”) force for each handling step (cap removal, dose setting and injection, see Figure 1). Two measurements were performed and recorded for each handling step and force level. Table 3 lists the force measurements performed during the study. Participants were randomly assigned to test the three handling steps in a cross-over design to control for order and learning effects.
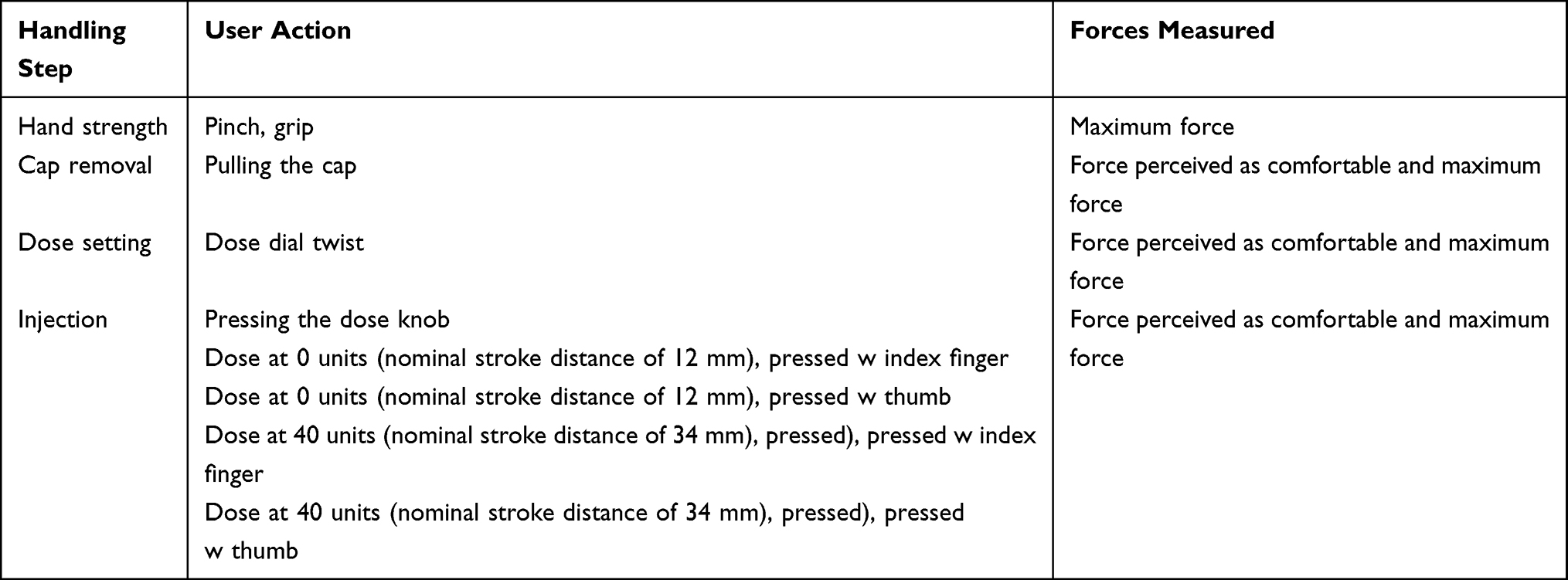 |
Table 3 Overview of Injection Pen Handling Steps and Force Measurements Covered in the Study |
Statistical Analysis
Power calculations to assess sample size were not performed. It was assumed that a minimum of 15 participants per group would be sufficient to collect force data from the testing procedure. Descriptive statistics were used to analyze the collected data. Inferential statistics were not performed.
Results
Force Data
Figure 2 presents the measured force data for participants’ hand strength, the force they considered comfortable, and their maximum for each handling step (cap removal, dose setting and injection). Figure 3 presents the measured force data for the injection handling step split between large and small dose and between thumb and index finger. The observed range of forces is quite wide for all types of measurements.
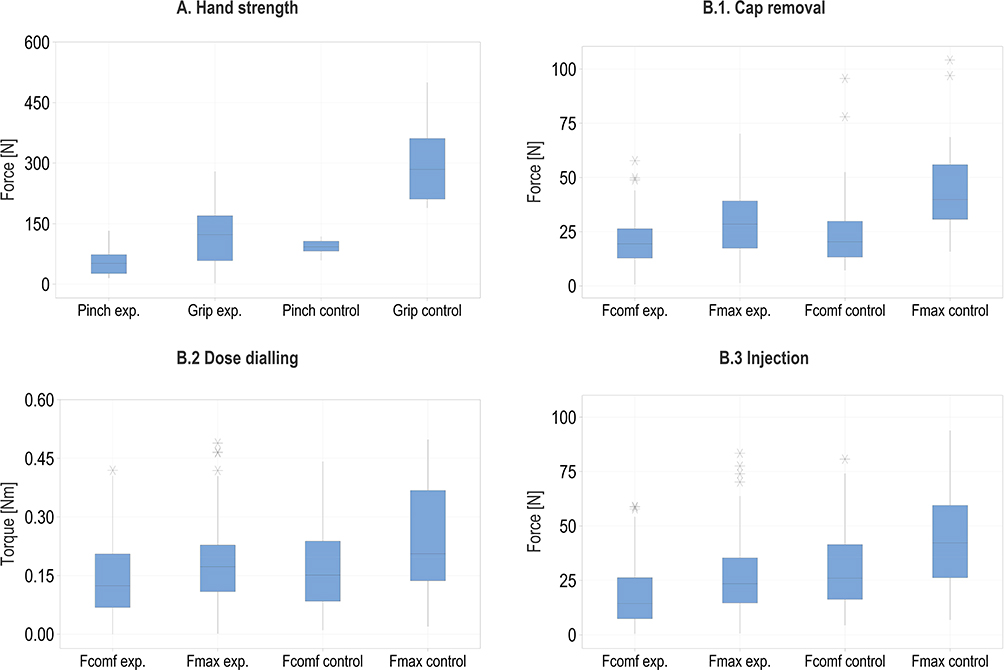 |
Figure 2 Force and torque sensor data for hand strength (A) and handling steps (B.1–B.3). Box plots are presented for all data points (two readings per participant and condition, n=31x2 for Experimental and n=15x2 for Control). For the injection handling step (B.3) the data shown is for all doses and grips (n=31x4 for Experimental and n=15x4 for Control). |
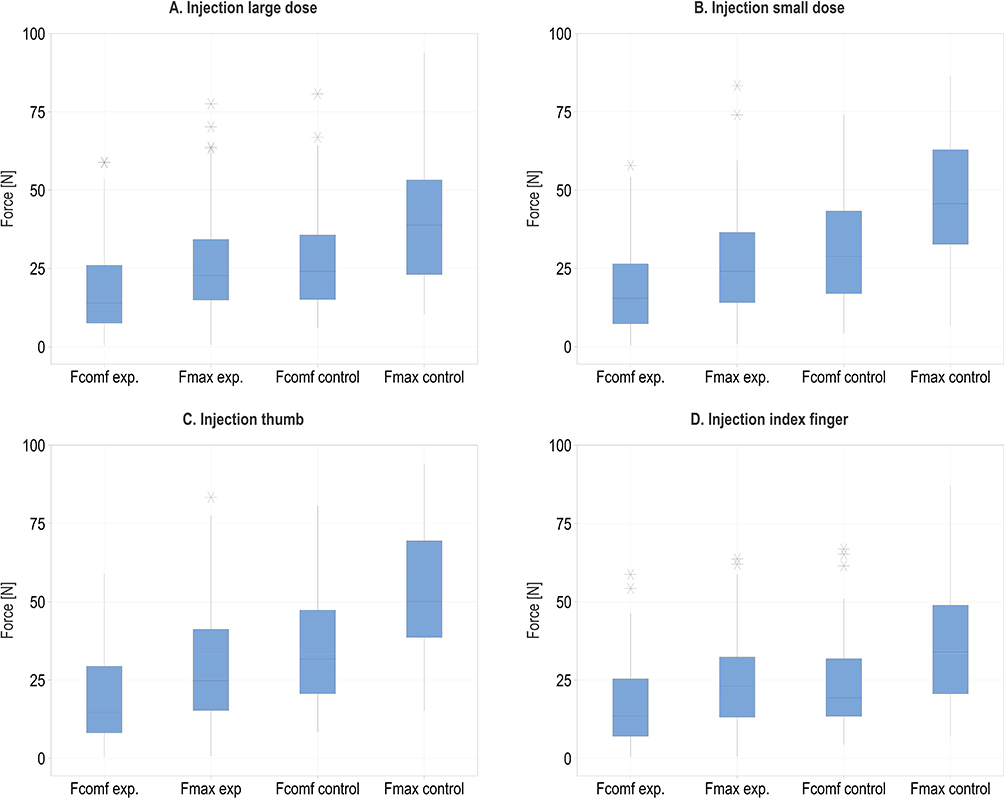 |
Figure 3 Force sensor data for the injection handling steps with large dose (A), small dose (B), thumb (C) and index finger (D). Box plots are presented for all data points (two readings per participant and condition, n=31x2 for Experimental and n=15x2 for Control). |
The data shows that the force levels of the control group participants were generally higher than those of the experimental group. Moreover, the maximum force or torque consistently exceeded the force levels that users perceived as comfortable. The simulations using thumb over index finger and for low over high dose injection resulted in higher observed forces.
Influence of Users’ Characteristics on Force
Figure 4 presents the measured hand strength and force and torque values for the different handling steps as a function of participant age. The hand strength, force levels perceived as comfortable, and maximum force levels for all types of handling steps all decrease with participants’ age. This decrease is most pronounced for grip strength. The tendency is similar for all handling steps and somewhat more pronounced for maximum force levels than for force levels considered comfortable.
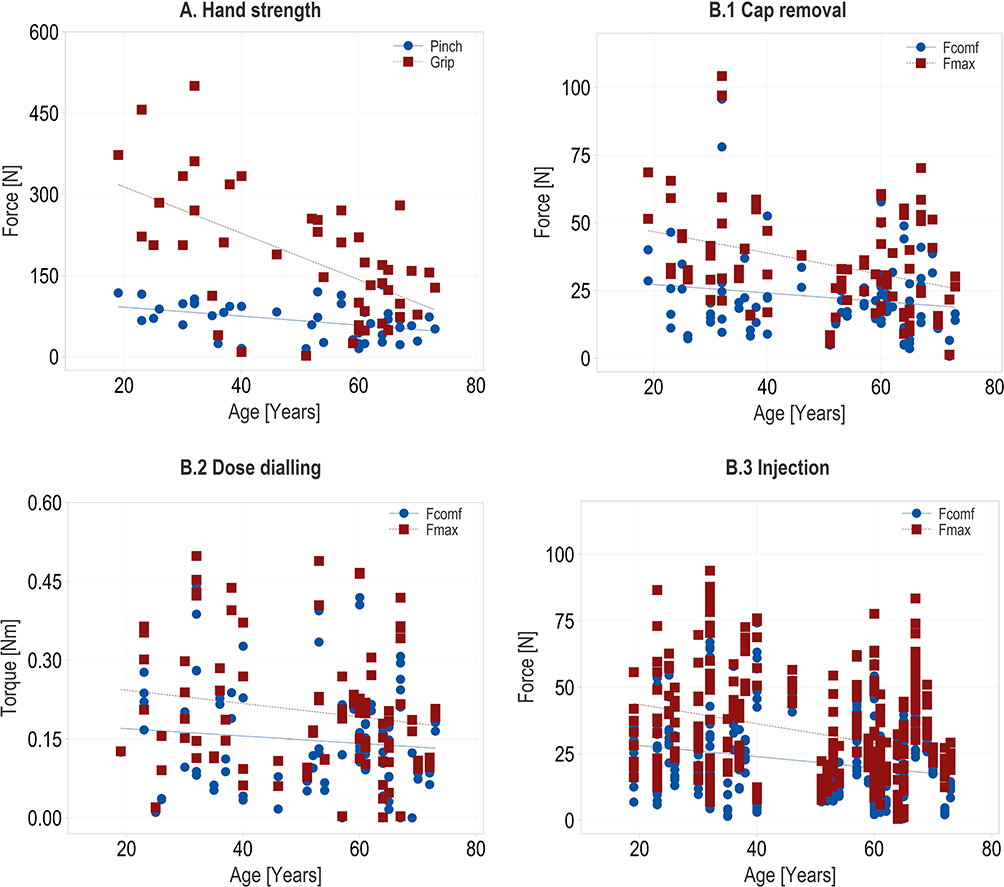 |
Figure 4 Relationship between age and hand strength (A). and relationship between age and perceived comfortable force (torque) and maximum force per device handling step (B.1–B.3). Each data point represents the average value of two individual measurements (n=46). |
Figure 5 shows the median values of hand strength, user forces, and torque based on participants’ M-SACRAH impairment score. Participants with impairments (M-SACRAH score) have lower grip and pinch strength than those without impairments (control), and these strengths decrease as the M-SACRAH score increases. The median values of user forces are generally lower for impaired participants than for healthy participants. However, there is no consistent relationship between the level of impairment and the observed force levels. The forces observed for cap removal and dose dialing slightly increases as impairment increases. In contrast, for injection, both the force perceived as comfortable and the maximum force tend to follow a U-shaped relationship with the M-SACRAH score, with a local minimum at a moderate M-SACRAH score.
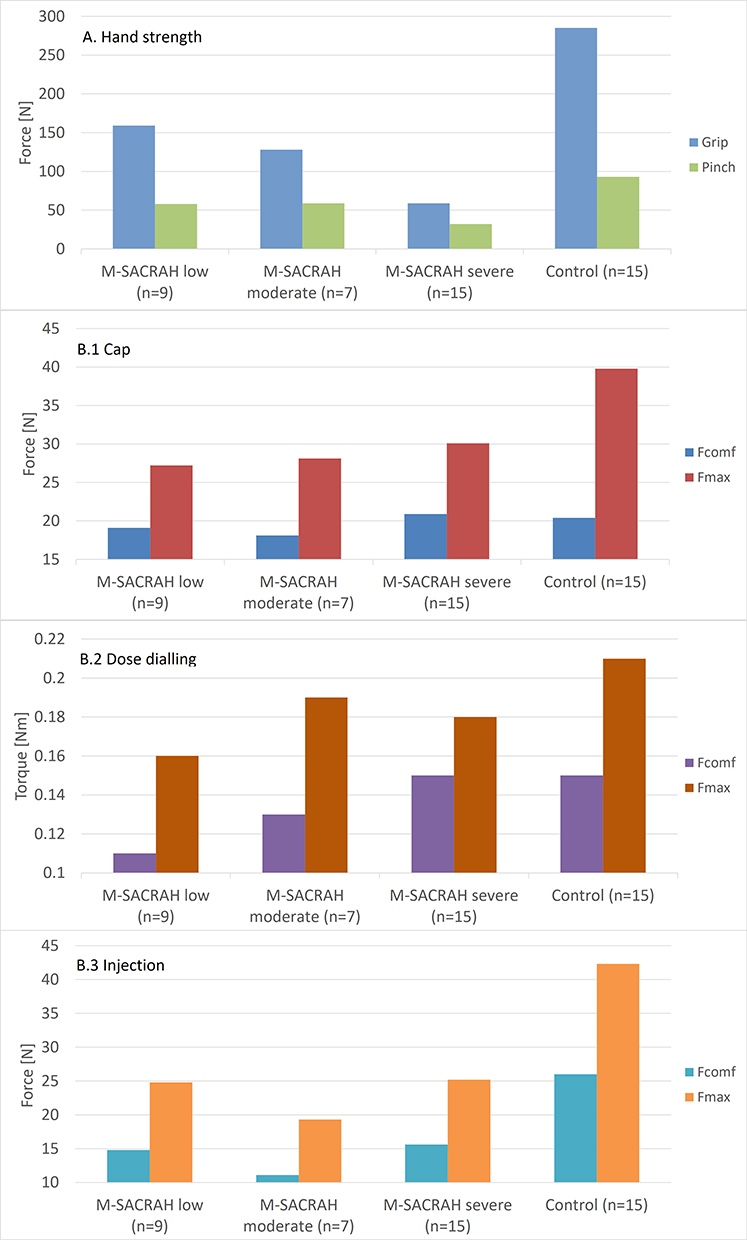 |
Figure 5 Relationship between dexterity impairment (M-SACRAH scores) and perceived comfortable force (torque) and force and maximum force for age (A) and for each device handling step (B.1–B.3). Each data point represents the median value of all measurements (two readings per participant and condition). |
Relationship Between Comfortable and Maximum Force
Figure 6 shows the relationship between perceived comfortable force and torque levels and their maximum for the different handling steps as a function of participant impairments. The ratio between comfortable and maximum force is highest for dose dialing, with values around 0.7 for participants with low or no impairment and 0.8 or above for the most impaired participants. For injection, the ratio remains constant at approximately 0.6 across all levels of impairment. For cap removal, the ratio is lowest (0.5) for unimpaired participants and then increases to about 0.7 for all impaired participants, regardless of impairment level.
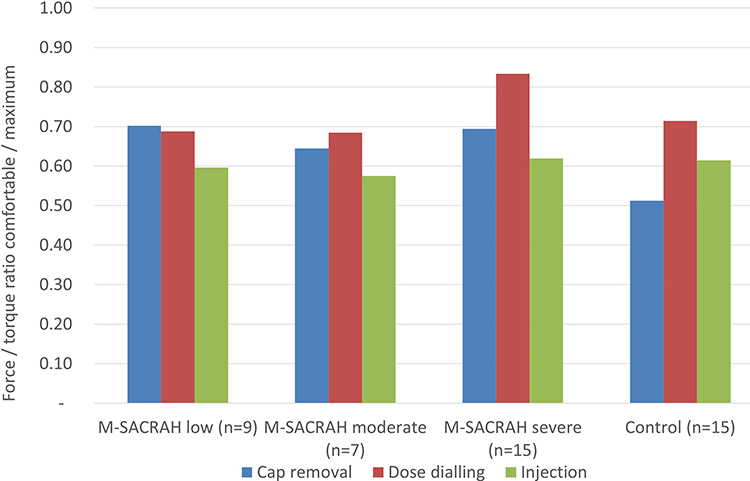 |
Figure 6 Ratio between the perceived comfortable force (torque) and the maximum force (torque) for the three handling steps. Each data point represents the ratio between the median values of all measured data points (two readings per participant and condition). |
Discussion
The critical findings that hand strength, perceived comfortable force levels, and maximum force levels decrease with age and impairment are consistent with results reported in the literature.33,35,36 Similarly, the measured force data show a broad variability, a phenomenon reported by previous studies. For example, past work on hand strength suggested a comparable variability when considering both male and female participants.34 These results provide initial evidence for the validity of the sensor-augmented simulated use study approach.
The baseline grip and pinch strength values obtained in this work are consistent with those reported in previous literature. For example, Puh’s study on healthy subjects reported grip strength values ranging from 100 to 700N and pinch strength values between 50 and 200N.34 The present study, which included healthy and impaired subjects, found a more significant decline with age than previous work (see Figure 4). This difference can be explained by the fact that most impaired participants included in the current study were over 50 years old, disproportionally impacting the results for older participants.
The force levels recorded during cap removal align with the data reported in the literature for de-capping autoinjectors.27 This study included healthy and impaired users and found that all participants could exert a minimum force of 56 N, which is the force required to remove the cap from the device with the highest force specification, and still achieve a 100% success rate. The present study reported maximum force levels of approximately 40N for the control and 29N for the experimental groups. The lower levels found in the current study may relate to differences in cap and device geometry, which resulted in different grips. The cap used in the autoinjector study27 was bigger and had design features that allowed for a better grip compared to the slim tubular pen cap used in the current study (see Figure 1).
No information regarding dialing torques for the use of injection devices was found in the literature. However, a study on handling forces of inhalers reported torque values between 0.5 and 1Nm for twisting movements for both actuations and user capability.37 These values are significantly higher than those observed in the current study, below 0.2Nm. This difference may be due to geometrical variations, as the inhalers were two to three times larger than the pens studied here, providing a much better grip than the pen dose dials.
Previous laboratory studies reported readings ranging from 5 to 30N for the force required to perform injections with pens similar in design to those included in the current study.6 It is important to note that higher forces were measured when injecting at high rates with thin needles, which is not typical during the actual use of such pens. The force levels perceived as comfortable identified in the current study are consistent with what patients would typically apply during actual injections, below 15N. The maximum push operating forces reported in the inhaler studies were 25 to 80N,27,38 similar to the maximum values observed in the current study – despite geometrical differences between the different inhalers and the pens. These findings imply that the push motion used for injection may be less sensitive to variations in geometry compared to the pull and twist motions required for the other handling steps.
It is widely accepted that impairment, as measured by the M-SACRAH score, is inversely correlated with hand strength and, therefore, affects the maximum forces a user can apply.35 The current study found that grip strength decreased by 50–80% and pinch strength by 40–70% when comparing healthy and impaired users. These values fall within the same range as the values of 45–55% found in a study by Dhara et al that compared the grip strength of healthy individuals to those with orthopedic challenges.36 No studies or data on the influence of impairment on handling forces of injection devices were found in the literature. Therefore, the study on inhalers37 was used for comparison. This study examined the push and twist actuation forces and torques of healthy and arthritic individuals. The results indicate that arthritic users applied maximum push forces approximately 30% lower than healthy adults and about 20% lower than healthy older individuals.37 The twisting torque values for arthritic users compared to healthy adults and older individuals were 50% and 30% lower, respectively. The present study revealed a comparable decrease in maximum force for cap removal and injection for impaired compared to healthy users, with a reduction of around 25% and 40%, respectively (cf. Figure 4). However, the observed decrease in torque between impaired and healthy users was only 15%. It is unclear why this difference with the inhaler data exists. However, it may again be related to the significant difference in size and geometry between the inhalers used in that study and the pen injector in the current study.
To the author’s knowledge, Schneider et al conducted the only study that provides data on the ratio of comfortable to maximum force for injection devices.27 The study found a ratio of approximately 0.6 between preferred and maximum force. Additionally, the study on inhalers37 can also be used as a comparison for actual forces required to use a device, assuming that the devices are designed for user comfort. The study on inhalers found that healthy adults have a ratio of 0.3 between their maximum force and the force required to operate the device, while arthritis patients have a ratio of 0.4. For pen injectors, the corresponding ratio for injection force is 0.3 for healthy adults and 0.5 for impaired users, based on an actuation force of 12 N and the maximum force values in Figure 5. The ratios between comfortable and maximum forces observed in the current study (ie, 0.5–0.8) are slightly higher than the ratios of maximum to actual actuation of the device. However, they are in good agreement with the ratio between maximum and comfortable force observed in the cap removal study.
It is important to consider the limitations of the study when interpreting these findings. The devices used in the study were mock-ups with sensors attached, and not complete, fully functional pen injectors. Therefore, the handling in terms of grip, movement, and travel during actuation may differ from that of real devices. Additionally, the study was based on simulated use rather than real injections, which may have also impacted the results. Furthermore, power calculations to assess sample size were not performed.
Conclusion
The study makes a significant contribution to the field of self-injection device design by addressing a critical gap in our understanding of handling forces during patient-device interactions. The research employed a sensor-augmented approach to simulated use studies and quantitatively assessed users’ self-reported comfortable and maximum force levels across handling steps. The study considered variations in user groups based on characteristics such as strength and dexterity. The findings indicate that were differences in both comfortable and maximum force levels between the control and patient groups. These levels also decreased slightly with user age and level of impairment, emphasizing the importance of customizing device specifications to suit diverse user characteristics. Additionally, the study suggests that device geometry and holding pattern can also affect force levels.
These findings highlight the significance of integrating quantitative data in the design and development of self-injection devices, going beyond conventional formative and summative usability studies. Sensor-augmented simulated use studies provide comprehensive insights that inform the definition of performance requirements and device specifications, facilitating the development of patient-centered injection devices.
Ethics Approval and Informed Consent
The study complied with the principles of the declaration of Helsinki. In agreement with the Institutional Review Board (Castle IRB, Chesterfield, USA) and the exemptions provided under 45 CFR 46.104, ethical approval was not considered necessary for this simulated human factors study as the participants only interacted with dummy devices and no correlations or conclusions on therapies were assumed. Furthermore, the study was not specific to the safety and effectiveness of any product, and risk was extremely minimal. Participants provided informed consent, and also consented to the publication of anonymized responses from the study.
Acknowledgments
The authors would like to express their gratitude to Michael Harkisheimer and Mary Yovanoff of Design Science in Philadelphia, UA, for conducting the study and creating an initial compilation of the data.
Disclosure
JL, AS and CJ are employees of Ypsomed AG. The authors have no other competing interests to report for this work.
References
1. Andre AD, Mohr J, Cornelius B, et al. Successful validation of a wearable, on-body infusor for subcutaneous administration of Furoscix® in heart failure patients, caregivers, and health care practitioners. J Card Fail. 2020;26(10):S68. doi:10.1016/j.cardfail.2020.09.199
2. Lange J, Schneider A, Jordi C, Lau M, Disher T. Formative study on the wearability and usability of a large-volume patch injector. Med Dev. 2021;14:363–377. doi:10.2147/MDER.S337670
3. Lageat C, Combedazou A, Ramus C, Guerrero K, Frolet C, Glezer S. Formative and validation human factors studies of a new disposable autoinjector for subcutaneous delivery of chronic disease therapies. Expert Opin Drug Delivery. 2021;18(11):1761–1775. doi:10.1080/17425247.2021.1954906
4. Klonoff DC, Bassock S, Dwyer A, et al. Evaluating the usability and safety of the semaglutide single-dose pen-injectors through summative (human factors) usability testing. J Diabetes Invest. 2021;12(6):978–987. doi:10.1111/jdi.13429
5. Andre A, Squittieri N, Patil SB. Evaluation of the octreotide acetate pen injector and its instructions for use in a formative human factors study. Adv Ther. 2021;38(6):3129–3142. doi:10.1007/s12325-021-01739-1
6. Schneider AE, Lange J. Pen devices for self-injection: contrasting measured injection force with users’ perceived ease of injection. Expert Opin Drug Delivery. 2018;15(2):115–125. doi:10.1080/17425247.2018.1415884
7. Privitera MB, Evans M, Southee D. Human factors in the design of medical devices–Approaches to meeting international standards in the European Union and USA. Appl Ergon. 2017;59:251–263. doi:10.1016/j.apergo.2016.08.034
8. Rojas KM, Cosler L, Santos DL. A Narrative Review of FDA Human Factors Validation Requirement: The Needs of Key Stakeholders and Proposal of an Industry (Human Factors Service Providers) Maturity Assessment Tool. Los Angeles, CA: SAGE Publications Sage CA; 2019:222–233.
9. Veasey R, Ruf CA, Bogatirsky D, et al. A review of reusable insulin pens and features of TouStar—a new reusable pen with a dedicated cartridge. Diabetol Metab Syndr. 2021;13(1):1–7. doi:10.1186/s13098-021-00763-z
10. Bohannon NJ, Ohannesian JP, Burdan AL, Holcombe JH, Zagar A. Patient and physician satisfaction with the Humulin/Humalog Pen, a new 3.0-mL prefilled pen device for insulin delivery. Clin Ther. 2000;22(9):1049–1067. doi:10.1016/S0149-2918(00)80084-3
11. Lange J, Richard P, Bradley N. Usability of devices for self-injection: results of a formative study on a new disposable pen injector. Med Dev. 2014;7:195–203. doi:10.2147/MDER.S63918
12. Lange J, Richard P, Bradley N. Usability of a new disposable autoinjector platform device: results of a formative study conducted with a broad user population. Med Devices. 2015;8:255–264. doi:10.2147/MDER.S85938
13. Barone DA, Singer BA, Merkov L, Rametta M, Suarez G. Survey of US patients with multiple sclerosis: comparison of the new electronic interferon Beta-1b Autoinjector (BETACONNECT) with mechanical autoinjectors. Neurol Ther. 2016;5(2):155–167. doi:10.1007/s40120-016-0047-3
14. Schneider A, Kolrep H, Horn H-P, Jordi C, Gierig S, Lange J. Understanding patient preferences for handheld autoinjectors versus wearable large-volume injectors. Expert Opin Drug Delivery. 2023;20(2):271–283. doi:10.1080/17425247.2022.2162037
15. Torjman MC, Machnicki R, Lessin J, et al. Evaluation of an investigational wearable injector in healthy human volunteers. Expert Opin Drug Deliv. 2017;14(1):7–13. doi:10.1080/17425247.2017.1252748
16. Weinhold T, Del Zotto M, Rochat J, Schiro J, Pelayo S, Marcilly R. Improving the safety of disposable auto-injection devices: a systematic review of use errors. AAPS Open. 2018;4(1):7. doi:10.1186/s41120-018-0027-z
17. Schiro J, Pelayo S, Heyndels L, Marcilly R Melles M, Albayrak A, GoossensRH. Design of an Evidence-Based Checklist to Help Prevent Use Errors with Auto-Injector Pens. Convergence: Breaking Down Barriers Between Disciplines. HEPS 2022. Springer Series in Design and Innovation. Springer 30 ; 2024:275–285.
18. Singer B, Wray S, Miller T, et al. Patient-rated ease of use and functional reliability of an electronic autoinjector for self-injection of subcutaneous interferon beta-1a for relapsing multiple sclerosis. Mult Scler Relat Disord. 2012;1(2):87–94. doi:10.1016/j.msard.2011.11.002
19. Tschiedel B, Almeida O, Redfearn J, Flacke F. Initial experience and evaluation of reusable insulin pen devices among patients with diabetes in emerging countries. Diabetes Ther. 2014;5(2):545–555. doi:10.1007/s13300-014-0081-z
20. Vermeire S, D’Heygere F, Nakad A, et al. Preference for a prefilled syringe or an auto-injection device for delivering golimumab in patients with moderate-to-severe ulcerative colitis: a randomized crossover study. Patient Preference Adherence. 2018;12:1193–1202. doi:10.2147/PPA.S154181
21. Goldstein HH. Pen devices to improve patient adherence with insulin therapy in type 2 diabetes. Postgrad Med. 2008;120(3):172–179. doi:10.3810/pgm.2008.09.1917
22. Buysman E, Conner C, Aagren M, Bouchard J, Liu F. Adherence and persistence to a regimen of basal insulin in a pre-filled pen compared to vial/syringe in insulin-naive patients with type 2 diabetes. Curr Med Res Opin. 2011;27(9):1709–1717. doi:10.1185/03007995.2011.598500
23. Hupperts R, Becker V, Friedrich J, et al. Multiple sclerosis patients treated with intramuscular IFN-beta-1a autoinjector in a real-world setting: prospective evaluation of treatment persistence, adherence, quality of life and satisfaction. Expert Opin Drug Deliv. 2015;12(1):15–25. doi:10.1517/17425247.2015.989209
24. Wang T, Conrad KA, van Brunt K, Rees TM. Attributes influencing insulin pen preference among caregivers and patients with diabetes who require greater than 20 units of mealtime insulin. J Diabetes Sci Technol. 2016;10(4):923–931. doi:10.1177/1932296816633232
25. McNamara M, Turner-Bowker DM, Westhead H, et al. Factors driving patient preferences for Growth Hormone Deficiency (GHD) Injection Regimen and Injection Device Features: a discrete choice experiment. Patient Preference Adherence. 2020;14:781. doi:10.2147/PPA.S239196
26. Nguyen H, Posner J, Kalsekar I, Ruggles J, Ruggles J. A discrete-choice experiment to quantify patient preferences for frequency of glucagon-like peptide-1 receptor agonist injections in the treatment of type 2 diabetes. Curr Med Res Opinion. 2016;32(2):251–262. doi:10.1185/03007995.2015.1117433
27. Schneider A, Richard P, Mueller P, Jordi C, Yovanoff M, Lange J. User-centric approach to specifying technical attributes of drug delivery devices: empirical study of autoinjector-cap removal forces. Patient Preference Adherence. 2021;15:159. doi:10.2147/PPA.S298725
28. Schneider A, Kolrep H, Jordi C, Richard P, Horn H-P, Lange J. How to prevent medication errors: a multidimensional scaling study to investigate the distinguishability between self-injection platform device variants. Expert Opin Drug Delivery. 2019;16(8):883–894. doi:10.1080/17425247.2019.1637852
29. US Food and Drug Administration; 2017 Docket FDA-2016-D-4412. Comparative Analyses and Related Comparative Use Human Factors Studies for a Drug-Device Combination Product Submitted in an ANDA
30. US Food and Drug Administration. Applying human factors and usability engineering to medical devices: guidance for industry and Food and Drug Administration staff. In: The Federal Register. US Food and Drug Administration; 2016:81.
31. Xiao X, Li W, Clawson C, Karvani D, Sondag P, Hahn JK. Evaluation of performance, acceptance, and compliance of an auto-injector in healthy and rheumatoid arthritic subjects measured by a motion capture system. Patient Preference Adherence. 2018;12:515–526. doi:10.2147/PPA.S160394
32. Schneider A, Mueller P, Jordi C, et al. Hold the device against the skin: the impact of injection duration on user’s force for handheld autoinjectors. Expert Opin Drug Delivery. 2020;17(2):225–236. doi:10.1080/17425247.2020.1704730
33. Puh U. Age-related and sex-related differences in hand and pinch grip strength in adults. Int J Rehabil Res. 2010;33(1):4–11. doi:10.1097/MRR.0b013e328325a8ba
34. Sautner J, Andel I, Rintelen B, Leeb BF. Development of the M-SACRAH, a modified, shortened version of SACRAH (Score for the Assessment and Quantification of Chronic Rheumatoid Affections of the Hands). Rheumatology. 2004;43(11):1409–1413. doi:10.1093/rheumatology/keh360
35. Stamm T, Mathis M, Aletaha D, Kloppenburg M, Machold K, Smolen J. Mapping hand functioning in hand osteoarthritis: comparing self‐report instruments with a comprehensive hand function test. Arthritis Care Res. 2007;57(7):1230–1237. doi:10.1002/art.22989
36. Dhara PC, De S, Pal A, Sengupta P, Roy S. Assessment of hand grip strength of orthopedically challenged persons affected with upper extremity. J Life Sci. 2009;1(2):121–127. doi:10.1080/09751270.2009.11885143
37. Ciciliani A-M, Langguth P, Wachtel H. Handling forces for the use of different inhaler devices. Int J Pharm. 2019;560:315–321. doi:10.1016/j.ijpharm.2019.01.053
38. Frohnhofen H, Hagen O. Handgrip strength measurement as a predictor for successful dry powder inhaler treatment. Zeitschrift für Gerontologie und Geriatrie. 2011;44(4):245–249. doi:10.1007/s00391-011-0222-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.