")
Back to Journals » Cancer Management and Research » Volume 15
The Progress of Platelets in Breast Cancer
Authors Wang L, Zhang K, Feng J, Wang D, Liu J
Received 24 April 2023
Accepted for publication 27 July 2023
Published 11 August 2023 Volume 2023:15 Pages 811—821
DOI https://doi.org/10.2147/CMAR.S418574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Luchang Wang,1,2 Kaijiong Zhang,3 Jia Feng,1 Dongsheng Wang,3 Jinbo Liu1
1Department of Laboratory Medicine, Affiliated Hospital of Southwest Medical University, Luzhou, 646000, People’s Republic of China; 2Department of Clinical Laboratory, Chengdu Second People’s Hospital, Chengdu, 610017, People’s Republic of China; 3Department of Clinical Laboratory, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, School of Medicine, University of Electronic Science and Technology of China, Chengdu, 610041, People’s Republic of China
Correspondence: Jinbo Liu, Department of Laboratory Medicine, Affiliated Hospital of Southwest Medical University, No. 5, Section 3, Zhongshan Road, Jiangyang District, Luzhou, Sichuan Province, 646000, People’s Republic of China, Tel +86 0830 3165120, Email [email protected]
Abstract: Breast cancer is the most common female cancer and the sixth leading cause of death, seriously affecting the quality of life of women. Platelets, one of the fragments derived from megakaryocytes, are being increasingly investigated by tumor researchers because of their anticoagulant function. According to relevant studies, platelets, as the key source of circulating angiogenesis-related factors, can regulate tumor angiogenesis and vascular integrity, and they can also affect the tumor microenvironment, thereby facilitating the proliferation and differentiation of tumor cells. By covering or transferring normal MHC I molecules to tumor cells, platelets can protect tumor cells from being killed by the immune system and facilitate tumor cell metastasis. However, details on the mechanisms involved have remained elusive. This paper reviews and analyzes studies of the role of platelets in tumorigenesis, tumor cell proliferation, tumor metastasis, and cancer treatment to provide readers with a better understanding of the relevant studies.
Keywords: breast cancer, platelets, angiogenesis, proliferation, metastasis
Introduction
Breast cancer was first documented in ancient Egypt. Since the 1970s, the incidence rate in Asian countries, which were previously considered areas with low breast cancer incidence, has increased year by year. Breast cancer (11.7%) had the highest incidence rate among women worldwide in 2020 according to world cancer statistics, replacing lung cancer (11.4%) as the most diagnosed cancer in the world.1 There is an increasing trend in incidence in both high and less developed regions, and the incidence in highly developed regions is generally 2–4 times higher than that in less developed regions.2 Despite the increasing prevalence, patients with breast cancer have a higher survival rate than those with more fatal cancers, probably because the breast tissue is excisable. According to statistics from 2013 to 2017, breast cancer incidence has increased by 0.5%, while the mortality rate has decreased by 1.0%.2,3 However, the mental and emotional disorders caused by major surgery, as well as death resulting from recurrence or metastasis, still endanger women’s health. Given the large population in China, the numbers of women with breast cancer and dying from breast cancer death there are the highest in the world, and these numbers continue to rise: the prevalence rate in China rose from 30.4 per million in 2015 to 41.6 per million in 2020, and the mortality rate rose from 15.6% in 2018 to 18% in 2020.4 Since the emergence of breast cancer, efforts have been made to explore its pathogenesis to find ways to eradicate the disease. Although the causes of breast cancer are unknown, significant progress has been made.
In recent years, the role of platelets in tumor treatment has received increasing attention from researchers, and thus, the role of platelets in breast cancer has been intensively studied by many breast cancer researchers. Platelets are one of the fragments derived from megakaryocytes. Their primary functions include coagulation and hemostasis, as well as protection of vascular endothelial cells, endothelial repair, and atherosclerosis prevention. Dense clusters of platelets contain large amounts of norepinephrine, adenosine diphosphate (ADP), and serotonin, which can be released in large quantities when platelets aggregate and become activated, leading to further recruitment of platelets and leukocytes and propagating the aggregation reaction.5 Alpha particles, in particular, store high levels of angiogenesis-related regulators, which play a role in regulating neovascularization and, as a result, can induce tissue repair or ischemic tissue revascularization.6 Platelet-derived microparticles (PMPs) are generated by platelets shedding from the plasma membrane through activation, replenishment, high shearing force, or apoptosis.7 Platelet activation increases intracellular calcium, which activates calpain, cytoskeletal proteins, and Rho kinases, resulting in cell contraction and the generation of membrane vesicles.8 Alternatively, resting platelets involved in αIIβ3 integrin-mediated actin cytoskeletal instability can also release particles independent of calpain activation.9 PMPs were originally thought to be “platelet dust” and are primarily derived from platelets. Particulates are classified according to the cell of origin based on surface antigen expression, and platelet-derived particulates are identified by surface expression of CD41 or CD42b.10 Studies have shown that PMPs are important for various physiological and pathophysiological signaling pathways and that they serve as a source of tissue factor (TF) and phosphatidylserine. PMPs are also involved in coagulation.11 Therefore, we aimed to review the mechanism of platelets in the development of breast cancer and its clinical application.
The Mechanism of Platelets in the Development of Breast Cancer
Thrombocytosis associated with solid tumors was first identified by Leopold Riess more than a century ago.12 Thrombocytosis can increase platelet baseline levels by up to 20 times through tumor-derived and systemic factors.13 Numerous studies have found a negative relationship between increased platelet counts and disease-specific survival in cancers such as lung, colon, breast, pancreatic, renal, and gynecologic cancers and melanoma and malignant glioblastoma.14 The ratio of platelets to lymphocytes can likewise be used as a factor for predicting diagnosis and prognosis for patients with tumors.15–18 Platelets can also facilitate rapid tumor growth by promoting tumor angiogenesis and the maintenance of tumor vascular integrity; they can affect tumor cell metastasis by facilitating epithelial-mesenchymal transition and assisting tumor cells in evading the killing and phagocytosis of host immune system cells (Figure 1). Therefore, the inclusion of platelet-based biomarkers in emerging “liquid biopsy” strategies for cancer patients has significant potential to improve diagnostic accuracy and prediction of treatment response.
 |
Figure 1 Tumor growth and tumor dormancy depend on factors regulating the “angiogenic switch” in tumors, and platelets are involved in tumor growth and metastasis. |
The Role of Platelets in Angiogenesis in Cancer
Tumor angiogenesis is generated by a complex network of tumor cells and cells of the tumor microenvironment, as well as cells recruited from the bone marrow to the tumor microenvironment.19 Secreted growth factors (eg, vascular endothelial growth factor (VEGF), FGF, PDGF, etc.) and their corresponding receptors (eg, Notch signaling receptors, integrins, etc.) enable the necessary intercellular communication.20 Platelets, as a key source of circulating angiogenesis-related factors, can regulate tumor angiogenesis and vascular integrity, and one of the most important angiogenic proteins is VEGF, which is transported and released by platelets.21 Ciccone22 and Sohn23 demonstrated by cell experiments that increasing levels of VEGF can activate the VEGF pathway, thereby facilitating the proliferation of breast tumor cells and tumor angiogenesis. Furthermore, platelet alpha (α) and dense (δ) granules contain and release proteins, lipids, growth factors, cytokines and proteases that directly or indirectly affect angiogenesis20 (Table 1) that can be actively taken up by platelets through endocytosis. Megakaryocytes selectively transfer some mRNAs and/or proteins to platelets,24 so platelets can actively synthesize proteins once stimulated. The release of different factors and proteins from platelet granules is largely dependent on the selective release of specific stimulated factors; for example, selective PAR-4 agonists stimulate the release of endothelin-containing granules, whereas selective PAR-1 agonists stimulate the release of VEGF-containing granules.25,26 VEGF is also released from platelets by ADP stimulation. ADP stimulation is inhibited by antagonizing P2Y1 and P2Y12 receptors but does not affect the release of the endothelial inhibitory hormone.27 In addition to regulating angiogenesis, platelets regulate vascular integrity and thus prevent tumor bleeding. The binding and interaction between released CXCL12 (SDF-1) and the receptors CXCR4 or CXCR7 cause the activation of various downstream signaling cascades (MAPK, PI3K/AKT, and NF-κB), recruiting hematopoietic progenitor cells and inducing endothelial cell activation to maintain hematologic reconstitution.28 The secretion of granules containing ANGPT1 and 5-hydroxytryptamine can help to maintain vascular integrity. These granules can stabilize tumor vessels via VEGF, which is derived from responding tumor cells.29 Platelets can also reduce tissue damage by regulating vascular integrity and inhibiting immune cell infiltration into tumors, thereby controlling cytokine release.30
 |
Table 1 Factors Released from Platelets That Affect Angiogenesis |
The Role of Platelets in Metastasis in Breast Cancer
A prerequisite for cancer metastasis is the survival of cancer cells in circulation. Normally, large numbers of circulating tumor cells (CTCs) are rapidly destroyed, but the interaction of tumor cells with platelets protects some CTCs from the cell death induced by TNFα31 and natural killer (NK) cells.32 Lopez et al33 experimentally demonstrated that mice lacking NK cells or NK cell effector molecules had a significantly higher metastatic burden of homozygous tumor cells delivered via different methods. There are five ways for tumor cells to evade the killing of NK cells (Figure 2). The first is the “immune decoy” mechanism, in which platelets induce tumor cells to release the necessary ligands (eg, NKG2D34 or TNF/TNF family receptor members), which allows tumor cells to avoid recognition by NK cells and thus inhibits NK cell degranulation and the production of IFNγ and other inflammatory cytokines. This mechanism effectively inhibits the immune clearance of tumor cells by NK cells. Shen et al35 confirmed the application of this mechanism in breast cancer. The second mechanism is platelet-derived TGFβ-mediated CD226/CD96-CD112/CD155 axis inhibition.36 Platelets further inhibit NK cells by suppressing surface CD226 and CD96 expression and the expression of their associated ligands on tumor cells. An example of the third mechanism is that NK cells that can infiltrate non-small-cell lung cancer (NSCLC) and breast cancer preferentially exhibit the CD56bright (CD27+CD11b− in mice, CD56bright in humans) phenotype common of immature NK cells, which suggests that certain NK cell subpopulations are selectively recruited to the tumor bed and are less cytotoxic than the CD56dim (CD27-CD11b+ in mice, CD56dim in humans) phenotype common of mature NK cells. Thus, lung and breast tumors may protect themselves from NK cell killing.32 The fourth mechanism is that cancer cells and platelets bind to mucins on the surface of cancer cells via GPIb-IX-V and GPIIb-IIIa mediated by tumor cell integrins αVβ3 or P-selectin and then create a partial physical barrier that protects tumor cells from NK cell killing.36 The fifth mechanism is that platelets can bind to the surface of tumor cells via “normal” MHC I molecules, preventing NK cells from recognizing tumor cells as foreign cells. As a result, NK cell cytotoxicity and IFN- production are limited.37
 |
Figure 2 The five ways for tumor cells to evade the killing of NK cells. (a) Members of the miR-17-92 in the platelet specifically downregulated NKG2DL (MICA/B and ULBP1/2/3) in tumor, which reduces the recognition and killing effects of NK cells; (b) the platelet-derived TGFβ inhibit the expression of CD226/CD96 in NK cells surface and their associated ligands (CD112/CD155) on tumor cells; which affects the binding of tumor cells to NK cells; (c) the upregulation of chemokines (CXCL9/CXCL10/CCL19) and acting on the receptors (CCR7/CXCR3) mainly expressed by CD56bright NK cells (immature NK cells) recruits massive immature NK cells; which influence the killing effect of mature NK cells on tumor cells; (d) platelets wrap around tumor cells to prevent NK cells kiling; (e) platelets transfer “normal” MHC I molecules to surface of tumor cells, which prevents NK cells from recognizing tumor cells. |
The interaction between tumor cells and microvascular endothelial cells occurs before successful extravasation and metastasis formation, which is critical in driving metastasis.38 In the absence of endothelial injury or activation, vascular endothelial cells remain quiescent. However, dysfunctional endothelial cells, including cells exposed to inflammation and vascular activation, trigger the upregulation of adhesion molecules and secretion of growth factors and cytokines and change vascular permeability, all of which facilitate tumor metastasis by promoting the adhesion of tumor cells to endothelial cells and endothelial cell migration.39 Hsu found that secretion of CXCL17 by breast cancer cells increased the accumulation of CD11b+Gr-1+ MDSCs in the lung, induced pulmonary angiogenesis through PDGF-BB, and facilitated tumor extravasation, colonization, and survival, and ultimately lung metastasis.40 Kassassir’s study revealed that the first and simplest evidence of platelet involvement in metastasis was the positive correlation between platelet count and the number of metastatic foci,41 confirming that platelet count may be a valuable predictor of cancer metastatic potential. Gareau experimentally confirmed that activated platelets can enhance the proliferation and metastatic potential of breast cancer cells.42 The mechanism is primarily mediated by ADP binding to the purinergic P2Y12 receptor on platelets. Yao et al showed that platelet TPM3 mRNA transfer into breast cancer cells via microvesicles can facilitate cancer cell migration.43 Liu et al demonstrated that diallyl trisulfide (DATS), a bioactive component of garlic, affects the proliferation and apoptosis of breast tumor cells by significantly blocking the platelet activation and aggregation induced by platelet-activating factor (PAF) and reducing thromboxane B2 (TXB2) production; furthermore, DATS inhibits the migration and invasion of MDA-MB-231 cells in the presence of PAF-activated platelets in vitro in a dose-dependent manner and significantly decreases the release of activated TGFβ1 from the platelet-tumor cell system.44 Leblanc et al showed that autotaxin (ATX), in association with fully active integrin αVβ3, controls the physiological level of lysophosphatidic acid (LPA) in the blood through its lysophospholipase D (lysoPLD) activity, thus participating in LPA-dependent breast cancer cell metastasis.45 Schito et al found that hypoxia-inducible factor (HIF-1) facilitates lymphatic metastasis of breast cancer through direct transactivation of the gene encoding platelet-derived growth factor B (PDGF-B), confirming the proliferative and chemotactic effects of PDGF-B on lymphatic vessel endothelial cells.46 For immune checkpoint therapy, targeting LAG3 and TIGIT and their ligands (LGALS3 and NECTIN2) is a potential therapeutic strategy for patients with liver and brain metastases from breast cancer.47
The Influence of Platelets on the Tumor Microenvironment
The tumor microenvironment plays a significant role in tumor progression and metastasis. Platelet-mediated secretion of soluble factors, such as chemokines and cytokines, growth factors, adhesion molecules, and receptors, is important for pericyte differentiation, proliferation, recruitment, and interaction with endothelial cells and affects fibroblast proliferation and the function of non-NK immune cells, thereby affecting tumor cell growth, proliferation, and metastasis. Zhang et al found that platelet-derived PDGF-B plays an important role in the malignant transformation of the tumor microenvironment and elucidated the role of the platelet-specific release of PDGF-B in tumor ECM remodeling for the first time.48 Patel et al demonstrated that PDGF-B stimulates collagenase activity during the remodeling phase of tissue repair and induces a “noninvasive” EMT characterized by loss of epithelial phenotype and cytoskeletal rearrangement but no cell mobilization or invasion of the sub embryonic space.49 The absence of cell invasion following PDGF-B-induced EMT may be due to a lack of gelatinase activity or inhibition of MMP2 and MMP9 activity. pADAM17 was shown to be associated with platelet activation by Zhou,50 and the degree of change in pADAM17 expression was found to be associated with clinical parameters of platelet activation in breast cancer, suggesting that downregulation of pADAM17 may be associated with tumor progression and metastasis. There is increasing evidence that multiple factors released by platelets induce EMT of tumor cells, including TGFβ, the most extensively researched factor. TGFβ-induced EMT of tumor cells primarily occurs via regulatory signaling pathways such as the Ras-Erk/PKMA, p38/MAPK, JNK, Rho-GTPase, PI3K/Akt, and Smad pathways.51 In addition, TGFβ can also mediate EMT by regulating miRNA transcription.52 LPA is mainly derived from lysophospholipids produced by thrombin-activated platelets and generated by the action of plasma lysoPLD, whose receptors LPA(1), LPA(2), and LPA(3) are expressed in human primary breast tumors and a series of human breast cancer cell lines.53 Boucharaba et al showed that local production of active LPA in the tumor microenvironment in vivo supports both the proliferation of LPA(1)-dependent breast cancer cells and LPA(1)-dependent secretion of IL-6 and IL-8, causing bone destruction.54 Shan confirmed that signaling mediated by PDGF-BB and PDGF-DD binding to PDGF receptor (PDGFR) is important for the survival and growth of metastatic breast cancer cells in the bone microenvironment.55
Clinical Application of Platelets in Breast Cancer
Application of Platelets in the Diagnosis of Breast Cancer
In addition to the initial diagnosis of cancer based on clinical manifestations, imaging reports, and blood tumor-related markers, the main tool for cancer diagnosis is still a pathological examination of tumor tissue. However, pathological examinations are almost always invasive, so screening for cancer-based on blood biomarkers has attracted increasing attention in the form of “liquid biopsy”. Such methods look for circulating tumor factors - a collection of circulating components derived from cancer tissue, including circulating tumor proteins, circulating tumor nucleic acids (circulating tumor DNA (ctDNA) and circulating tumor RNA (ctRNA)), CTCs, extracellular vesicles (EVs), and tumor-educated platelets (TEPs).56 Cancer-associated platelets are now recognized as a promising indicator that can be used in liquid biopsy. New data suggest that platelet-based biomarkers may be more useful for diagnosis than other biomarkers.57 Platelets actively absorb and accumulate additional biological substances during their lifetimes, which may include substances released by tumor cells as extracellular bodies.58 Therefore, platelets are rich in RNAs, of which miRNAs are the most abundant. In platelets, miRNAs play important roles in regulating the induction of protein recombination, splicing, and transcription and the repression of platelet protein expression.59 TEPs are platelets with altered RNA profiles due to the influence of tumors and can carry a large amount of tumor-associated RNA and protein information because they bind with signaling molecules and their receptors. In 2015, Best et al60 prospectively obtained platelets from a large number of healthy blood donors and treated and untreated patients with early, localized, or advanced metastatic cancer and sequenced them with RNA-seq; the analysis identified 5003 differentially expressed protein-coding and noncoding RNAs in platelets from patients with six types of cancer compared with those from healthy donors. Using this information, the researchers distinguished patients with localized and metastatic tumors from healthy individuals with 96% accuracy. Furthermore, the platelet spectrum appeared to be sufficiently tumor-type specific so that in most cases, the primary source of disease could be correctly identified. In many cases, the platelet RNA profiles accurately predicted oncogene expression or mutation status in many tumors, including MET or HER2 positivity and KRAS, EGFR, or PIK3CA mutation. Later, Best et al used a particle swarm optimization (PSO) enhancement algorithm based on different gene sets in a platelet RNA sequencing library to diagnose early and late non-small cell lung cancer (NSCLC) with accuracies of 81% and 88%, respectively.61 Thus, the platelet gene set can be characteristically altered not only by the release of biomolecules induced by cancer cells and the tumor microenvironment (stromal and immune cells) but also by changing the vesicle-mediated transport mechanism by which nucleic acids and proteins are physiologically exchanged with other platelets, immune cells, endothelial cells, and tumor cells.
The platelet proteome may be an equally suitable source of diagnostic and predictive biomarkers for tumors. Platelets contain a large number of TGFβ than other cells and are known to be the largest reservoir of VEGF in the body, containing more than 95% of the total VEGF content in healthy adults.62 In cancer patients, platelet VEGF concentrations are significantly higher than those in other relevant body parts (6.5- to 28.2-fold) and even higher than that in the tumor itself. Platelets may take up VEGF produced by other cellular sources, including tumor cells because VEGF concentrations in platelets increase over time as long as VEGF sources are present.63 Thus, thrombocytosis may be an ominous prognosis, as it represents a massive expansion of the VEGF-carrying capacity in the body. Karsten et al compared clinical features (a: before adjuvant chemotherapy, b: four weeks after treatment, c: two years after treatment) of 205 patients who had undergone primary breast surgery with those of healthy controls (n=107). They found that in the breast cancer cohort, VEGF-A plasma concentrations were significantly higher at all time points examined and lower after treatment. Two years after chemotherapy, VEGF-A levels were associated with increased cancer-related mortality, whereas VEGF165b levels were significantly higher. The VEGF-A/VEGF-A165b ratio was lower after chemotherapy, and the level of circulating VEGF-A165b in women with primary breast cancer was significantly reduced.64 Clinical studies have also shown elevated levels of platelet angiogenesis regulators in patients with cancer (breast, colorectal, prostate, kidney, or ovarian cancer or lymphoma) compared to healthy controls, and these factors include VEGF, ANGPT-1, MMP2, platelet factor-4 (PF-4), and PDGF.65 Therefore, fluctuations in the platelet proteome may be a surrogate marker of tumor activity.
Application of Platelets in Breast Cancer Treatment
Integrin Glycoprotein Family Receptors
Platelet glycoprotein (GP) receptors mediate platelet adhesion, activation, and aggregation, and many GP receptors exist as noncovalently linked heterodimers, including those belonging to the α and β subunit integrin families.66 Under physiological conditions, platelet adhesion and activation are triggered by thrombin production upon tissue factor or endothelial cell exposure to the subendothelial matrix when activation/injury occurs. Early platelet adhesion is regulated through the interaction of GPIbα with the von Willebrand factor (VWF) and the binding of integrins to collagen. These GP receptors act synergistically with thrombin signaling through PARs to activate platelets. After platelets are activated, the GPIIb/IIIa (integrin αIIbβ3) conformation changes from a low-affinity to a high-affinity state, and high-affinity GPIIb-IIIa binds fibrinogen, accelerating interplatelet bridge formation and thrombus formation.67 Given that all these GP receptors regulate platelet-tumor cell interactions, blocking them may be an effective anticancer strategy. Through cell experiments, Kononczuk et al demonstrated that abciximab and eptifibatide can induce MCF-7 cell apoptosis via the expression of proline oxidase (POX), the signaling molecules ERK 1/2, transcription factors (NF-κB), HIF-1α, and VEGF; DNA and collagen biosynthesis; and prolinase activity, and eptifibatide induced stronger effects than abciximab.68
P-Selectin Receptors
P-selectin is found in platelet alpha granules and is expressed on activated platelets and endothelial cells, whereas E-selectin and L-selectin are constitutively expressed on endothelial cells and leukocytes and are involved in vascular cell adhesion in the interaction between leukocytes, platelets, and endothelial cells. Their receptors are mostly oligosaccharides, which can be modified by glycosylation and have been linked to malignant cell transformation.69 According to experimental data, platelets and cancer cell surface mucin bind in a P-selectin-dependent manner and contribute to platelet tumor microembolus formation and tumor cell extravasation via a process similar to leukocyte migration via endothelial cells.70 Given the existence of P-selectin-dependent platelet tumor cell interactions, Jafari et al actively targeted P-selectin with fucoidan-doxorubicin nanoparticles (FU-Dox-NPs) developed by direct conjugation of doxorubicin (Dox) to a fucoidan backbone. They found that the active targeting of P-selectin by FU-Dox-NPs enhanced the cellular uptake and cytotoxicity of the MDA-MB-231 cell line with high P-selectin expression compared to the MDA-MB-468 cell line with low P-selectin expression.71 P-selectin is widely used to specifically bind targeted drug nanoparticles to tumor tissues via the high-affinity interactions between P-selectin, normally found on platelet membranes, and CD44 receptors on tumor cells, and this strategy can achieve efficient tumor treatment with reduced side effects.72–74
Protease-Activated Prothrombin Receptors and Antithrombin Methods
Protease-activated receptors (PARs) are a family of four-transmembrane G protein-coupled receptors that are activated by the most potent platelet agonists thrombin (PAR-1, PAR-3, and PAR-4) and trypsin-like serine protease (PAR-2).75 Human platelets express two thrombin-triggered PARs, namely, high-affinity PAR-1 and low-affinity PAR-4, whose functions may induce platelet angiogenesis and selective release of mitogenic regulators in addition to triggering platelet aggregation. [37,176,005] Related studies have shown that selective PAR-4 agonists stimulate the release of endothelial inhibitor-containing granules, whereas VEGF-containing granules are released after stimulation with selective PAR-1 agonists.25,26 Ray et al induced activation and overexpression of PAR-1 in breast cancer cells (EAC) by hemagglutinin protease (HAP) secreted by Vibrio cholerae. This activation and overexpression caused nuclear translocation of p50-p65 and p38 phosphorylation, which triggered activation of the NFκB and MAP kinase signaling pathways and increased the level of cytosolic reactive oxygen species in malignant cells, thereby inducing apoptosis.76 The experimental data of Thabet et al support the role of piroxicam and sulforaphane sulfide in inhibiting inflammation-driven breast cancer progression, and the researchers identified RAS and PAR-4 signaling as promising new therapeutic targets.77 Kim et al adopted GB83 (an inhibitor of PAR-2) to inhibit PKC-mediated MMP-9 expression and the metastatic ability in MCF-7 cells. Their experiments confirmed that downregulation of matrix proteases inhibited 12-O-tetradecanoylphorbol-13-acetate (TPA)-induced MMP-9 expression and invasiveness through PAR-2/PLCγ2/PKC/MAPK activation.78 The thrombin inhibitor hirudin reduced platelet-derived VEGF at thrombus sites by nearly 50% and inhibited tumor metastasis in an experimental model.79 Low molecular weight heparin(LMWH) inhibits the release of platelet angiogenic proteins mediated by tumor cells. For immune reaction, repeated administration of heparin may trigger heparin to induce thrombocytopenia and thrombosis (HIT/T) syndrome, which is closely related to the formation of deep vein thrombosis in limbs. If not recognized, it may endanger life. Despite preclinical studies showing significant effects on tumors, thrombin inhibitors inhibit PAR activity in host and tumor cells, which may lead to serious side effects, such as bleeding, making the development and usage of related drugs challenging.
Other Treatments
Platelets contain alpha and dense granules, which are rich in proteins, lipids, growth factors, cytokines, and proteases that affect angiogenesis, and platelets actively take up and sequester these factors via endocytosis. The different factors and proteins in these platelet granules depend mainly on the selective release of factors in response to specific stimuli; for example, the release and aggregation of platelet α granules are regulated through protein kinase C (PKC) α and β signaling. Moncada et al found that Ro32-0432 (a highly selective small molecule inhibitor of PKCα) preferentially inhibited the secretion of angiogenic regulatory molecules in α granules but not platelet aggregation, thus limiting platelet-stimulated angiogenesis, implying that the effect of platelets on tumor angiogenesis can be mitigated pharmacologically while maintaining hemostasis.80 The P2Y12 receptor is the primary receptor for ADP-stimulated platelet glycoprotein IIb/IIIa receptor activation. According to studies, ATP activates P2Y2R through inflammatory bodies, especially by regulating the inflammatory body components NLRC4, ASC, caspase-1, and Notch-4, to induce breast tumor invasion and angiogenesis.81,82 Clopidogrel (Plavix), which is a P2Y12 receptor antagonist, and some newly developed P2Y11 inhibitors, such as prasugrel and ticagrelor, are mostly used in the treatment of vascular disease, with little information in tumor treatment.
The Future of Targeted Platelet Therapy
The successful development of therapeutics that intervene in platelet-cancer cell interactions must strike a balance between inhibiting platelet-specific targets that play a role in cancer progression and maintaining normal platelet haemostatic function. In contrast, we have limited knowledge of the different stimulatory conditions for platelet mitogenic, pro- or anti-angiogenic, pro-inflammatory, anti-inflammatory and adhesion functions. We also do not know which specific platelet activities are most relevant to the malignant process and to what extent such interventions would compromise the essential physiological role of platelets in maintaining haemostasis. Current anti-platelet drugs target platelet receptors, their binding ligands, signalling proteins or soluble mediators of platelet function. Although drugs that block cyclooxygenases (eg aspirin), the ADP receptor P2Y12 (clopidogrel) and GPIIb/IIIa (abciximab) are the most widely used, their effects on cells other than platelets make it difficult to conclude that their anti-tumour properties are due exclusively to platelet inhibition. For example, the off-target effects of small molecule GPIIb/IIIa receptor inhibitors are mainly related to their inhibitory effect on the inflammatory response. This may likewise be a factor in the benefit of certain patients. Thus, the variable response and off-target effects of antiplatelet agents could explain the conflicting observations regarding the effects of antiplatelet agents on cancer incidence and survival. As antiplatelet agents continue to evolve, critically assessing their risk-benefit curves in an oncology context will make the use of the drugs more challenging.
Conclusion
The roles of platelets and thrombocytosis in facilitating tumor growth and metastasis were first proposed by Gasic83 in 1968, and the depth of our understanding of the relevant mechanisms has increased. Platelets not only infiltrate the tumor microenvironment and interact directly with cancer cells but also protect CTCs from the lethal attack of the immune system and other proapoptotic stimuli in the circulation and contribute to CTC attachment to the endothelium, providing signals to establish a premetastatic niche. Platelets can even reduce the effectiveness of chemotherapy and other targeted therapies in cancer patients. To avoid serious complications, an approach that specifically targets platelet-tumor cell interactions while not interfering with normal platelet function is a promising direction for breast cancer treatment. Therefore, studying platelets and their effects on the coagulation system and surface receptors and their uptake and release functions will help to elucidate the role of platelets in metastatic dissemination and tumorigenesis. In recent years, bioinformatic analysis has advanced rapidly, and the adoption of bioinformatic approaches to analyze the favorable and unfavorable effects of platelets on cancer will undoubtedly aid the development and improvement of selectively targeted interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung HA, Ferlay J, Siegel RA, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Islami F, Ward EM, Sung H, et al. Annual report to the nation on the status of cancer, part 1: national cancer statistics. J Natl Cancer Inst. 2021;113(12):1648–1669.
3. Zhao Y, Zhu J, Zhang X, et al. Integrated IMRT vs segmented 3D-CRT of the chest wall and supraclavicular region for breast cancer after modified radical mastectomy: an 8-year follow-up. J Cancer. 2021;12(5):1548–1554. doi:10.7150/jca.51125
4. Cao W, Chen H-D, Yu Y-W, Li N, Chen W-Q. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J. 2021;134(7):783–791. doi:10.1097/CM9.0000000000001474
5. Crowley ST, Dempsey EC, Horwitz KB, Horwitz LD. Platelet-induced vascular smooth muscle cell proliferation is modulated by the growth amplification factors serotonin and adenosine diphosphate. Circulation. 1994;90(4):1908–1918. doi:10.1161/01.CIR.90.4.1908
6. Alanazi JS, Alqahtani FY, Aleanizy FS, et al. MicroRNA-539-5p-Loaded PLGA nanoparticles grafted with iRGD as a targeting treatment for choroidal neovascularization. Pharmaceutics. 2022;14(2):243. doi:10.3390/pharmaceutics14020243
7. Goubran HA, Burnouf T, Stakiw J, Seghatchian J. Platelet microparticle: a sensitive physiological “fine tuning” balancing factor in health and disease. Transfus Apher Sci. 2015;52(1):12–18. doi:10.1016/j.transci.2014.12.015
8. Fox JE, Austin CD, Boyles JK, Steffen PK. Role of the membrane skeleton in preventing the shedding of procoagulant-rich microvesicles from the platelet plasma membrane. J Cell Biol. 1990;111(2):483–493. doi:10.1083/jcb.111.2.483
9. Cauwenberghs S, Feijge MAH, Harper AGS, Sage SO, Curvers J, Heemskerk JWM. Shedding of procoagulant microparticles from unstimulated platelets by integrin-mediated destabilization of actin cytoskeleton. FEBS Lett. 2006;580(22):5313–5320. doi:10.1016/j.febslet.2006.08.082
10. George JN, Pickett EB, Saucerman S, et al. Platelet surface glycoproteins. Studies on resting and activated platelets and platelet membrane microparticles in normal subjects, and observations in patients during adult respiratory distress syndrome and cardiac surgery. J Clin Invest. 1986;78(2):340–348. doi:10.1172/JCI112582
11. Freyssinet JM, Toti F. Formation of procoagulant microparticles and properties. Thromb Res. 2010;125(1):S46–48. doi:10.1016/j.thromres.2010.01.036
12. Riess L. Zur pathologischen Anatomie des Blutes. Arch Anat Physiol Wissensch Med. 1872;1872:237–249.
13. Haemmerle M, Stone RL, Menter DG, Afshar-Kharghan V, Sood AK. The platelet lifeline to cancer: challenges and opportunities. Cancer Cell. 2018;33(6):965–983.
14. Buergy D, Wenz F, Groden C, Brockmann MA. Tumor-platelet interaction in solid tumors. Int J Cancer. 2012;130(12):2747–2760.
15. Anwar SL, Cahyono R, Avanti WS, Budiman HY, Harahap WA, Aryandono T. Pre-treatment neutrophil-lymphocyte and platelet-lymphocyte ratios as additional markers for breast cancer progression: a retrospective cohort study. Ann Med Surg. 2021;63:102144. doi:10.1016/j.amsu.2021.01.092
16. Hurmuz P, Ozyigit G, Kilickap S, et al. Gemcitabine based trimodality treatment in patients with muscle invasive bladder cancer: may neutrophil lymphocyte and platelet lymphocyte ratios predict outcomes? Urol Oncol. 2021;39(6):368.e19–368.e29. doi:10.1016/j.urolonc.2020.11.006
17. Lin J, Zhang W, Huang Y, et al. Sarcopenia is associated with the neutrophil/lymphocyte and platelet/lymphocyte ratios in operable gastric cancer patients: a prospective study. Cancer Manag Res. 2018;10:4935–4944.
18. Wang Y, Tang Y, Gao X, et al. Optimization of prostate cancer patient lymph node staging via the integration of neutrophil-lymphocyte ratios, platelet-lymphocyte ratios, and Ga-PSMA-PET-derived SUVmax values. Prostate. 2022;82(15):1415–1421. doi:10.1002/pros.24415
19. Kerbel RS. Tumor angiogenesis. N Engl J Med. 2008;358:2039–2049. doi:10.1056/NEJMra0706596
20. Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature. 2011;473(7347):298–307. doi:10.1038/nature10144
21. Möhle R, Green D, Moore MA, Nachman RL, Rafii S. Constitutive production and thrombin-induced release of vascular endothelial growth factor by human megakaryocytes and platelets. Proc Natl Acad Sci U S A. 1997;94(2):663–668. doi:10.1073/pnas.94.2.663
22. Ciccone V, Terzuoli E, Donnini S, Giachetti A, Morbidelli L, Ziche M. Stemness marker ALDH1A1 promotes tumor angiogenesis via retinoic acid/HIF-1α/VEGF signalling in MCF-7 breast cancer cells. J Exp Clin Cancer Res. 2018;37(1):311.
23. Sohn EJ, Jung D-B, Lee H, et al. CNOT2 promotes proliferation and angiogenesis via VEGF signaling in MDA-MB-231 breast cancer cells. Cancer Lett. 2018;412:88–98. doi:10.1016/j.canlet.2017.09.052
24. Cecchetti L, Tolley ND, Michetti N, Bury L, Weyrich AS, Gresele P. Megakaryocytes differentially sort mRNAs for matrix metalloproteinases and their inhibitors into platelets: a mechanism for regulating synthetic events. Blood. 2011;118(7):1903–1911. doi:10.1182/blood-2010-12-324517
25. Italiano JE, Richardson JL, Patel-Hett S, et al. Angiogenesis is regulated by a novel mechanism: pro- and antiangiogenic proteins are organized into separate platelet alpha granules and differentially released. Blood. 2008;111(3):1227–1233. doi:10.1182/blood-2007-09-113837
26. Jiang L, Luan Y, Miao X, et al. Platelet releasate promotes breast cancer growth and angiogenesis via VEGF-integrin cooperative signalling. Br J Cancer. 2017;117(5):695–703. doi:10.1038/bjc.2017.214
27. Bambace NM, Levis JE, Holmes CE. The effect of P2Y-mediated platelet activation on the release of VEGF and endostatin from platelets. Platelets. 2010;21(2):85–93. doi:10.3109/09537100903470298
28. Zhao K, Yao Y, Luo X, et al. LYG-202 inhibits activation of endothelial cells and angiogenesis through CXCL12/CXCR7 pathway in breast cancer. Carcinogenesis. 2018;39(4):588–600. doi:10.1093/carcin/bgy007
29. Ho-Tin-Noé B, Goerge T, Cifuni SM, Duerschmied D, Wagner DD. Platelet granule secretion continuously prevents intratumor hemorrhage. Cancer Res. 2008;68(16):6851–6858. doi:10.1158/0008-5472.CAN-08-0718
30. Ho-Tin-Noé B, Carbo C, Demers M, Cifuni SM, Goerge T, Wagner DD. Innate immune cells induce hemorrhage in tumors during thrombocytopenia. Am J Pathol. 2009;175(4):1699–1708. doi:10.2353/ajpath.2009.090460
31. Philippe C, Philippe B, Fouqueray B, Perez J, Lebret M, Baud L. Protection from tumor necrosis factor-mediated cytolysis by platelets. Am J Pathol. 1993;143(6):1713–1723.
32. Mattiola I. Immune circuits to shape natural killer cells in cancer. Cancers. 2021;13(13):3225. doi:10.3390/cancers13133225
33. López-Soto A, Gonzalez S, Smyth MJ, Galluzzi L. Control of Metastasis by NK Cells. Cancer Cell. 2017;32(2):135–154. doi:10.1016/j.ccell.2017.06.009
34. Cluxton CD, Spillane C, O’Toole SA, Sheils O, Gardiner CM, O’Leary JJ. Suppression of Natural Killer cell NKG2D and CD226 anti-tumour cascades by platelet cloaked cancer cells: implications for the metastatic cascade. PLoS One. 2019;14(3):e0211538. doi:10.1371/journal.pone.0211538
35. Shen J, Pan J, Du C, et al. Silencing NKG2D ligand-targeting miRNAs enhances natural killer cell-mediated cytotoxicity in breast cancer. Cell Death Dis. 2017;8(4):e2740. doi:10.1038/cddis.2017.158
36. Kim YJ, Borsig L, Varki NM, Varki A. P-selectin deficiency attenuates tumor growth and metastasis. Proc Natl Acad Sci U S A. 1998;95(16):9325–9330. doi:10.1073/pnas.95.16.9325
37. Placke T, Örgel M, Schaller M, et al. Platelet-derived MHC class I confers a pseudonormal phenotype to cancer cells that subverts the antitumor reactivity of natural killer immune cells. Cancer Res. 2012;72(2):440–448. doi:10.1158/0008-5472.CAN-11-1872
38. Mensah SA, Harding IC, Zhang M, et al. Metastatic cancer cell attachment to endothelium is promoted by endothelial glycocalyx sialic acid degradation. AiChE J. 2019;65(8). doi:10.1002/aic.16634
39. Blazejczyk A. Endothelium and cancer metastasis: perspectives for antimetastatic therapy.Pharmacol. Rep. 2015;67(4):711–718.
40. Hsu Y-L, Yen M-C, Chang W-A, et al. CXCL17-derived CD11bGr-1 myeloid-derived suppressor cells contribute to lung metastasis of breast cancer through platelet-derived growth factor-BB. Breast Cancer Res. 2019;21(1):23. doi:10.1186/s13058-019-1114-3
41. Kassassir H, Karolczak K, Siewiera KM, Wojkowska DW, Braun M, Watala CW. Time-dependent interactions of blood platelets and cancer cells, accompanied by extramedullary hematopoiesis, lead to increased platelet activation and reactivity in a mouse orthotopic model of breast cancer - implications for pulmonary and liver metastasis. Aging. 2020;12(6):5091–5120. doi:10.18632/aging.102933
42. Gareau AJ, Brien C, Gebremeskel S, Liwski RS, Johnston B, Bezuhly M. Ticagrelor inhibits platelet-tumor cell interactions and metastasis in human and murine breast cancer. Clin Exp Metastasis. 2018;35(1–2):25–35. doi:10.1007/s10585-018-9874-1
43. Yao B, Qu S, Hu R, et al. Delivery of platelet TPM3 mRNA into breast cancer cells via microvesicles enhances metastasis. FEBS Open Bio. 2019;9(12):2159–2169. doi:10.1002/2211-5463.12759
44. Liu Y, Zhao Y, Wang Y, et al. Suppressive role of diallyl trisulfide in the activated platelet-mediated hematogenous metastasis of MDA-MB-231 human breast cancer cells. Int J Mol Med. 2017;39(6):1516–1524. doi:10.3892/ijmm.2017.2953
45. Leblanc R, Lee S-C, David M, et al. Interaction of platelet-derived autotaxin with tumor integrin αVβ3 controls metastasis of breast cancer cells to bone. Blood. 2014;124(20):3141–3150. doi:10.1182/blood-2014-04-568683
46. Schito L, Rey S, Tafani M, et al. Hypoxia-inducible factor 1-dependent expression of platelet-derived growth factor B promotes lymphatic metastasis of hypoxic breast cancer cells. Proc Natl Acad Sci U S A. 2012;109(40):E2707–E16. doi:10.1073/pnas.1214019109
47. Zou Y, Ye F, Kong Y, et al. The single-cell landscape of intratumoral heterogeneity and the immunosuppressive microenvironment in liver and brain metastases of breast cancer. Adv Sci. 2023;10(5):e2203699. doi:10.1002/advs.202203699
48. Zhang Y, Manouchehri Doulabi E, Herre M, et al. Platelet-Derived PDGFB promotes recruitment of cancer-associated fibroblasts, deposition of extracellular matrix and Tgfβ signaling in the tumor microenvironment. Cancers. 2022;14:8.
49. Patel P, West-Mays J, Kolb M, Rodrigues J-C, Hoff CM, Margetts PJ. Platelet derived growth factor B and epithelial mesenchymal transition of peritoneal mesothelial cells. Matrix Biol. 2010;29(2):97–106. doi:10.1016/j.matbio.2009.10.004
50. Zhou Y, Heitmann JS, Kropp KN, et al. Regulation of platelet-derived ADAM17: a biomarker approach for breast cancer? Diagnostics. 2021;11(7). doi:10.3390/diagnostics11071188
51. Nelson KM, Weiss GJ. MicroRNAs and cancer: past, present, and potential future. Mol Cancer Ther. 2008;7:3655–3660. doi:10.1158/1535-7163.MCT-08-0586
52. Guo R, Hao G, Bao Y, et al. MiR-200a negatively regulates TGF-β-induced epithelial-mesenchymal transition of peritoneal mesothelial cells by targeting ZEB1/2 expression. Am J Physiol Renal Physiol. 2018;314(6):F1087–F95. doi:10.1152/ajprenal.00566.2016
53. Wang J, Sun Y, Qu J, Yan Y, Yang Y, Cai H. Roles of LPA receptor signaling in breast cancer. Expert Rev Mol Diagn. 2016;16(10):1103–1111. doi:10.1080/14737159.2016.1238763
54. Boucharaba A, Serre C-M, Grès S, et al. Platelet-derived lysophosphatidic acid supports the progression of osteolytic bone metastases in breast cancer. J Clin Invest. 2004;114(12):1714–1725. doi:10.1172/JCI200422123
55. Shan H, Takahashi T, Bando Y, Izumi K, Uehara H. Inhibitory effect of soluble platelet-derived growth factor receptor β on intraosseous growth of breast cancer cells in nude mice. Cancer Sci. 2011;102(10):1904–1910. doi:10.1111/j.1349-7006.2011.02026.x
56. De Rubis G, Krishnan SR, Bebawy M. Circulating tumor DNA - Current state of play and future perspectives. Pharmacol Res. 2018;136:35–44. doi:10.1016/j.phrs.2018.08.017
57. Chi KR. The tumour trail left in blood. Nature. 2016;532:269–271. doi:10.1038/532269a
58. D’Ambrosi S, Nilsson RJ, Wurdinger T. Platelets and tumor-associated RNA transfer. Blood. 2021;137(23):3181–3191. doi:10.1182/blood.2019003978
59. Miao S, Zhang Q, Chang W, Wang J. New insights into platelet-enriched miRNAs: production, functions, roles in tumors, and potential targets for tumor diagnosis and treatment. Mol Cancer Ther. 2021;20(8):1359–1366. doi:10.1158/1535-7163.MCT-21-0050
60. Best MG, Sol N, Kooi I, et al. RNA-Seq of tumor-educated platelets enables blood-based pan-cancer, multiclass, and molecular pathway cancer diagnostics. Cancer Cell. 2015;28(5):666–676. doi:10.1016/j.ccell.2015.09.018
61. Best MG, Sol N, Vancura A, et al. Swarm intelligence-enhanced detection of non-small-cell lung cancer using tumor-educated platelets. Cancer Cell. 2017;32(2):238–252.e9. doi:10.1016/j.ccell.2017.07.004
62. Karolczak K, Watala C. Blood platelets as an important but underrated circulating source of TGFβ. Int J Mol Sci. 2021;22(9):4492. doi:10.3390/ijms22094492
63. Kut C, Mac Gabhann F, Popel AS. Where is VEGF in the body? A meta-analysis of VEGF distribution in cancer. Br J Cancer. 2007;97(7):978–985. doi:10.1038/sj.bjc.6603923
64. Karsten MM, Beck MH, Rademacher A, et al. VEGF-A165b levels are reduced in breast cancer patients at primary diagnosis but increase after completion of cancer treatment. Sci Rep. 2020;10(1):3635. doi:10.1038/s41598-020-59823-5
65. Yan M, Lesyk G, Radziwon-Balicka A, Jurasz P. Pharmacological regulation of platelet factors that influence tumor angiogenesis. Semin Oncol. 2014;41(3):370–377. doi:10.1053/j.seminoncol.2014.04.007
66. Tesfamariam B, Wood SC. Targeting glycoprotein VI to disrupt platelet-mediated tumor cell extravasation. Pharmacol Res. 2022;182:106301. doi:10.1016/j.phrs.2022.106301
67. Li Z, Delaney MK, O’Brien KA, Du X. Signaling during platelet adhesion and activation. Arterioscler Thromb Vasc Biol. 2010;30(12):2341–2349. doi:10.1161/ATVBAHA.110.207522
68. Kononczuk J, Surazynski A, Czyzewska U, et al. αIIbβ3-integrin ligands: abciximab and eptifibatide as proapoptotic factors in MCF-7 human breast cancer cells. Curr Drug Targets. 2015;16(13):1429–1437. doi:10.2174/1389450115666140804220441
69. Qi C, Li B, Guo S, et al. P-Selectin-mediated adhesion between platelets and tumor cells promotes intestinal tumorigenesis in Apc(Min/+) mice. Int J Biol Sci. 2015;11(6):679–687. doi:10.7150/ijbs.11589
70. Läubli H, Borsig L. Selectins promote tumor metastasis. Semin Cancer Biol. 2010;20(3):169–177. doi:10.1016/j.semcancer.2010.04.005
71. Jafari M, Sriram V, Xu Z, Harris GM, Lee J-Y. Fucoidan-doxorubicin nanoparticles targeting P-selectin for effective breast cancer therapy. Carbohydr Polym. 2020;249:116837. doi:10.1016/j.carbpol.2020.116837
72. Li L, Fu J, Wang X, et al. Biomimetic “nanoplatelets” as a targeted drug delivery platform for breast cancer theranostics. ACS Appl Mater Interfaces. 2021;13(3):3605–3621. doi:10.1021/acsami.0c19259
73. Ye H, Wang K, Wang M, et al. Bioinspired nanoplatelets for chemo-photothermal therapy of breast cancer metastasis inhibition. Biomaterials. 2019;206:1–12. doi:10.1016/j.biomaterials.2019.03.024
74. Zhao W, Li T, Long Y, et al. Self-promoted albumin-based nanoparticles for combination therapy against metastatic breast cancer via a hyperthermia-induced “platelet bridge”. ACS Appl Mater Interfaces. 2021;13(22):25701–25714. doi:10.1021/acsami.1c04442
75. Zhao P, Metcalf M, Bunnett NW. Biased signaling of protease-activated receptors. Front Endocrinol. 2014;5:67. doi:10.3389/fendo.2014.00067
76. Ray T, Pal A. PAR-1 mediated apoptosis of breast cancer cells by V. cholerae hemagglutinin protease. Apoptosis. 2016;21(5):609–620. doi:10.1007/s10495-016-1229-2
77. Thabet NA, El-Guendy N, Mohamed MM, Shouman SA. Suppression of macrophages- Induced inflammation via targeting RAS and PAR-4 signaling in breast cancer cell lines. Toxicol Appl Pharmacol. 2019;385:114773. doi:10.1016/j.taap.2019.114773
78. Kim J-M, Park J, Noh E-M, et al. Downregulation of matriptase suppresses the PAR-2/PLCγ2/PKC-mediated invasion and migration abilities of MCF-7 breast cancer cells. Oncol Rep. 2021;46(6). doi:10.3892/or.2021.8198
79. Sierko E, Wojtukiewicz MZ. Inhibition of platelet function: does it offer a chance of better cancer progression control? Semin Thromb Hemost. 2007;33:712–721. doi:10.1055/s-2007-991540
80. Moncada de la Rosa C, Radziwon-Balicka A, El-Sikhry H, et al. Pharmacologic protein kinase Cα inhibition uncouples human platelet-stimulated angiogenesis from collagen-induced aggregation. J Pharmacol Exp Ther. 2013;345(1):15–24. doi:10.1124/jpet.112.200881
81. Jin H, Kim HJ. NLRC4, ASC and caspase-1 are inflammasome components that are mediated by P2YR activation in breast cancer cells. Int J Mol Sci. 2020;21(9):3337. doi:10.3390/ijms21093337
82. Kim DC, Jin H, Lee JS, Son E, Lee GW, Kim HJ. P2YR has a significant correlation with Notch-4 in patients with breast cancer. Oncol Lett. 2020;20(1):647–654. doi:10.3892/ol.2020.11630
83. Gasic GJ, Gasic TB, Stewart CC. Antimetastatic effects associated with platelet reduction. Proc Natl Acad Sci USA. 1968;61:46–52. doi:10.1073/pnas.61.1.46
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A 5`-tRNA Derived Fragment NamedtiRNA-Val-CAC-001 Works as a Suppressor in Gastric Cancer
Zheng J, Li C, Zhu Z, Yang F, Wang X, Jiang P, Yan F
Cancer Management and Research 2022, 14:2323-2337
Published Date: 4 August 2022
The Notch Signaling Pathway Contributes to Angiogenesis and Tumor Immunity in Breast Cancer
Jiang N, Hu Y, Wang M, Zhao Z, Li M
Breast Cancer: Targets and Therapy 2022, 14:291-309
Published Date: 27 September 2022
ITGB1BP1, a Novel Transcriptional Target of CD44-Downstream Signaling Promoting Cancer Cell Invasion
Ahmad SMS, Nazar H, Rahman MM, Rusyniak RS, Ouhtit A
Breast Cancer: Targets and Therapy 2023, 15:373-380
Published Date: 24 May 2023
Identification and Validation of Novel Metastasis-Related Immune Gene Signature in Breast Cancer
Ma S, Hao R, Lu YW, Wang HP, Hu J, Qi YX
Breast Cancer: Targets and Therapy 2024, 16:199-219
Published Date: 12 April 2024
Guanine-Rich RNA Sequence Binding Factor 1 Deficiency Promotes Colorectal Cancer Progression by Regulating PI3K/AKT Signaling Pathway
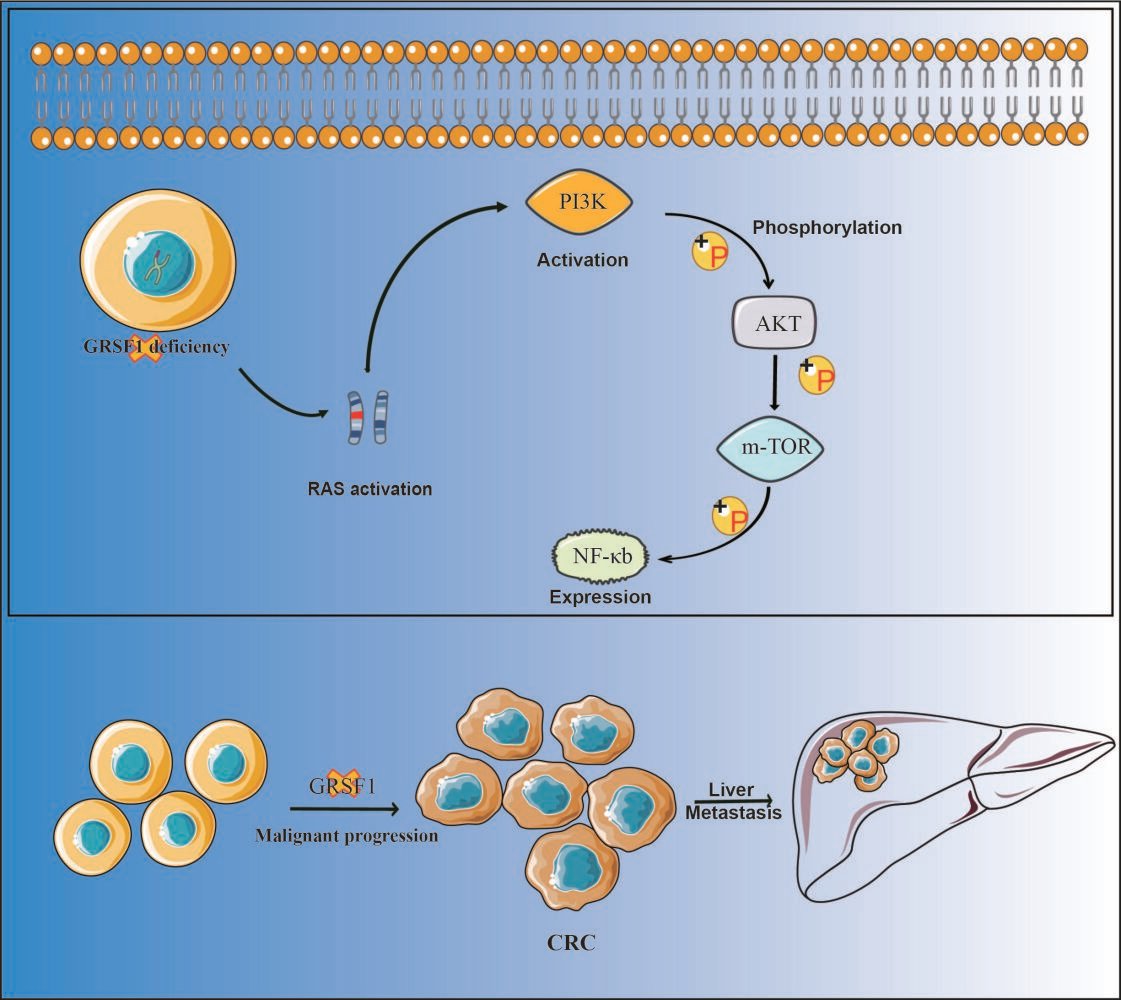
Huang J, Liu J, Lan J, Sun J, Zhou K, Deng Y, Liang L, Liu L, Liu X
Cancer Management and Research 2024, 16:629-638
Published Date: 11 June 2024